


The definition of crowned dens syndrome (CDS) is based on clinical findings such as acute onset of severe neck pain, restriction of neck motion, and fever, along with radiologic findings of calcification around the odontoid process [1].
The prevalence of CDS in patients with acute onset of severe neck pain is 2%, which is a rare disease [2,3]. Because the clinical manifestations of the syndrome are various, including neck pain, occipital or temporal headache, mandibular pain, facial pain, pharyngeal pain, and shoulder pain, among others, differentiation of CDS from other diseases may be difficult.
We describe a case of CDS in a 48-year-old woman with acute onset of severe neck, facial, and pharyngeal pain markedly provoked by swallowing, accompanied by fever, misdiagnosed as glossopharyngeal neuralgia.
CASE REPORT
A 48-year-old woman presented to our pain clinic reporting right neck and right facial and pharyngeal pain with acute onset one week earlier. There was no history of trauma or medical illness. Six days earlier, she had been referred to a general hospital for treatment owing to fever and elevated inflammatory markers on tests performed at a local clinic. Four days earlier, tests of inflammatory markers and brain computed tomography (CT) performed at the SMG-SNU Boramae Medical Center showed nonspecific findings.
When the patient first visited our clinic, her blood pressure was 115/62 mmHg, heart rate was 72/min, and body temperature was 37.9┬░C. She reported neck pain and facial and pharyngeal pain characterized as electric-like shooting, prickling, and burning pain aggravated by swallowing. She had no sensory changes or motor weakness. Under the suspicion of glossopharyngeal neuralgia, the patient was given a right glossopharyngeal nerve block with 1% lidocaine 50 mg and betamethasone 2 mg. She also received oral gabapentin 900 mg per day, a combination of tramadol 18.75 mg/acetaminophen 162.5 mg twice a day, and nortriptyline 5 mg at night. For differential diagnosis with tumors or anatomical abnormalities, facial CT was planned, with follow-up one week later.
At the second visit one week later, facial CT showed a 1.3 cm calcified mass near the odontoid process and right C1-2 facet joint (Fig. 1).
Fig.┬Ā1
Coronal (A), axial (B) and sagittal (C) computed tomography scan. Arrow: calcified mass in right posterolateral aspect of odontoid process at level of C1-2.

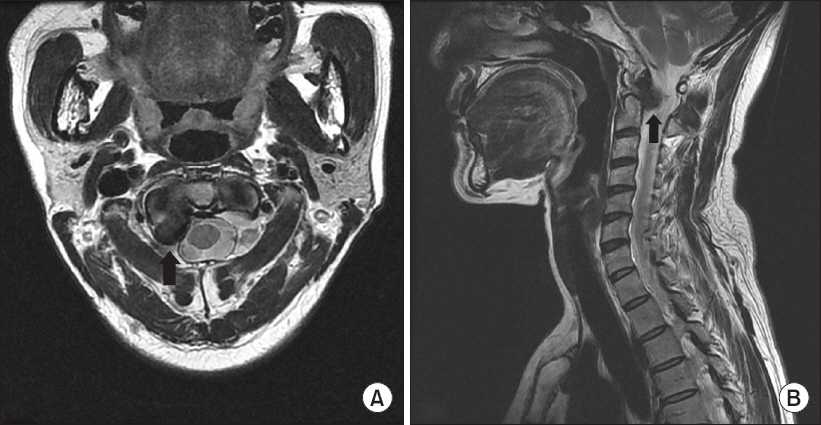
The diagnosis of CDS was made with radiologic findings of periodontoid calcification and clinical findings of acute onset of severe neck pain with fever. Cervical magnetic resonance imaging (MRI) was performed to confirm involvement of the nerve root and thecal sac, and to rule out malignancies. Cervical MRI showed a T2-dark signal intensity calcified mass, 1.3 cm, near the right C1-2 facet joint, with compression of the right C2 nerve root and thecal sac (Fig. 2).
Fig.┬Ā2
Axial (A) and sagittal (B) T2 magnetic resonance imaging. Arrow: T2-dark signal intensity calcified mass, 1.3 cm, near right C1-2 facet joint, with compression of right C2 nerve root and thecal sac.
At that time, the patient reported an improvement in pain of 80-90% since the glossopharyngeal nerve block, and she had no fever. Accordingly, no additional blood tests were performed. However, the right occipital pain persisted. Occipital compartment block was therefore performed with 1% lidocaine 50 mg and betamethasone 2 mg.
At the third visit a week later, the occipital pain was resolved. The patient was able to continue pain-free without medication, with no further sequelae.
DISCUSSION
CDS was first reported in 1985 by Bouvet et al. [4]. The calcifications appeared in a shape like a crown on the head of the odontoid process. However, 10% of cases of CDS do not show radiological ŌĆ£crowningŌĆØ of the odontoid process, despite the name. The positional relationship between the odontoid process and the calcification reported by Goto et al. [2] was as follows: calcium pyrophosphate dihydrate (CPPD) deposition may be posterior only (50%), posterolateral (27.5%), circular (12.5%), or anterior (5%). In 90% of cases of CDS, the calcification is located behind the odontoid process [2,3]. In the present case, the calcification was confirmed in the right posterolateral aspect of the odontoid process (Fig. 1).
From a retrospective review of 40 patients with CDS reported by Goto et al. [2], there were more women than men as 15 patients were men and 25 patients were women. CDS predominantly affected patients more than the age of 60. All of patients showed acute onset and appeared positive inflammatory sign such as fever, increased C-reactive protein level or erythrocyte sedimentation rate. Twenty two patients had history of pseudogout attack in other parts such as knees, wrists, or ankles, among others and 26 patients had chondrocalcinosis in other parts [2].
ŌĆśPseudogoutŌĆÖ is the acute synovitis due to CPPD deposition. Any joint may be affected, but knees and wrists are the most common sites. Acute pseudogout of neck, known as crowned dens syndrome, is a rare disease that CPPD crystals deposit in periodontoid tissues [3,5].
Periodontoid CPPD deposits are mostly due to unknown causes, but sometimes result from metabolic conditions including hypomagnesemia, hemochromatosis, hyperparathyroidism, and WilsonŌĆÖs disease [5].
The diagnosis of CDS is based on clinical features of acute attacks of cervico-occipital stiffness and severe neck pain with fever, along with radiological findings of calcifications near the odontoid process [4,6]. However, the clinical manifestations of CDS may be various, including neck pain, neck stiffness, shoulder weakness, shoulder pain, occipital or temporal headache, and facial pain, among others. In addition, CDS may be misdiagnosed as meningitis because it is often accompanied by fever and elevation of inflammatory markers. When patients report neck stiffness with pain in the shoulder girdle and jaw claudication or temporal headache, physicians may think of polymyalgia rheumatica or temporal arteritis instead of CDS [6]. In this case, the patient was misdiagnosed with glossopharyngeal neuralgia because her presentation included neck pain and facial and pharyngeal pain markedly provoked by swallowing. In patients with acute neck pain, the clinical features of CDS should be well recognized to avoid invasive and risky investigations such as lumbar puncture and temporal artery biopsy, long-term use of steroids due to misdiagnosis, and the use of antibiotics or surgery.
CT scan is the gold standard for the diagnosis of CDS [6-8]. However, the presence of periodontoid calcification on CT imaging is not diagnostic of CDS, and there may be asymptomatic calcification. Asymptomatic calcification in periodontoid tissues may occur in patients with inflammatory rheumatoid diseases such as ankylosing spondylitis and psoriatic arthritis [1,9]. The atlantoaxial joint is the most common site of rheumatoid arthritis [10]. CT imaging is better than MRI to assess calcifications in periodontoid tissues. CT scan is also useful for differential diagnosis of unidentified odontoid fractures [6].
The prognosis of CDS is good. The symptoms disappear within several weeks and the CPPD depositions can be absorbed [4,7,11]. Conservative treatments such as analgesics and colchicine may be helpful. Some authors have reported that the combination of non-steroidal anti-inflammatory drugs and steroids is the most effective treatment [4,6]. In this case, the patient obtained favorable results with steroid injection and a combination of tramadol/acetaminophen and gabapentin for pain relief.
In conclusion, CDS typically presents with clinical features of acute onset of severe neck pain accompanied by fever. However, many other symptoms may be present, and the spectrum of CDS is widening. In these patients, unnecessary or invasive investigation, and high-risk treatment or long-term use of medications such as steroids can be avoided if physicians are aware of CDS and make diagnoses based on CT imaging, although CDS is a rare disease.




