





Contralateral tension pneumothorax during one-lung ventilation (OLV) is a rare event. As this condition can rapidly lead to a life-threatening situation, early diagnosis and immediate treatment are important. However, signs of tension pneumothorax such as hypoxemia, increased airway pressure or hypotension [1], occur frequently during OLV, often leading to delayed diagnosis. In the present work, we report a case of a patient with sudden cardiovascular collapse due to tension pneumothorax on the contralateral lung during OLV for lobectomy. The patient was kept on extra-corporeal membrane oxygenation (ECMO) support until the cause of respiratory and hemodynamic failure was identified and recovered. We obtained informed consent from patient.
CASE REPORT
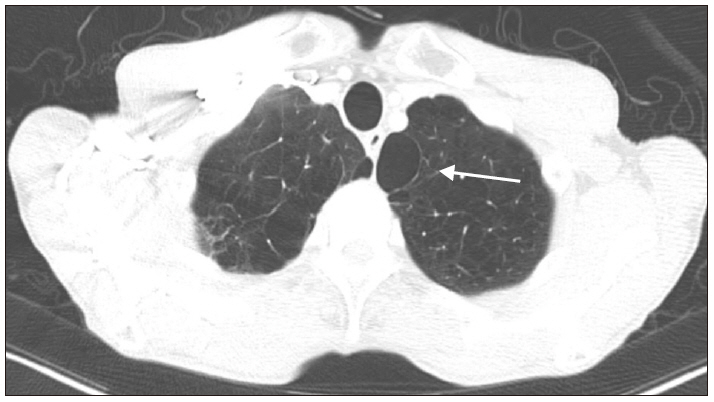
A 75-year-old male weighing 50 kg and having a height of 165 cm was scheduled to undergo right upper lobectomy for the treatment of non-small cell lung cancer. His significant medical history was chronic obstructive pulmonary disease (COPD) and was a 55-pack-year smoker. The preoperative pulmonary function test showed a moderate obstructive pattern with a forced expiratory volume of 1.64 L (61% of predicted) in one second. The chest computerized tomography revealed subsegmental atelectasis in bilateral lower lobes and right middle lobe, emphysema with bullae in bilateral lungs (Fig. 1), and scanty right pleural effusion. An electrocardiogram (ECG) performed before the surgery showed right bundle branch block, and transthoracic echocardiography revealed normal left ventricle (LV) global systolic function (ejection fraction [EF] = 58%) and abnormal relaxation of LV filling pattern.
Fig. 1
Chest computed tomography shows emphysema with bullae in the bilateral lung. Arrow indicates the large bulla on the left lung.
The patient received 0.2 mg of glycopyrrolate intramuscularly as a premedication. On arrival in the operating room, intraoperative monitoring was performed including ECG, non-invasive blood pressure, pulse oximetry, bispectral index, and capnography. The immediate preoperative vital signs of the patient were as follows: systolic/diastolic blood pressure of 112/74 mmHg, a heart rate of 90 beats/min, and Oxygen saturation (SpO2) of 96%. After preoxygenation with 100% oxygen, general anesthesia was induced with intravenous 70 mg of propofol, 20 mg of lidocaine, and continuous infusion of remifentanil. After confirming adequate mask ventilation, 60 mg of succinylcholine was given to facilitate passage of a double-lumen endotracheal tube (DLT), after which neuromuscular blockade was maintained with intermittent boluses of intravenous rocuronium. The trachea was intubated with a 37 Fr. left-side DLT (Mallinckrodt™, Covidien Inc., Ireland) under direct laryngoscopy. The DLT position was confirmed by chest auscultation and fiberoptic bronchoscopy. A left radial artery catheter and a central venous catheter were placed via the right internal jugular vein. Arterial blood gas analysis (ABGA) during two-lung ventilation (FiO2 0.6/end-tidal CO2 concentration [EtCO2], 34 mmHg) revealed pH 7.369, PaCO2 40.6 mmHg, PaO2 256.3 mmHg, and SaO2 99.8%. The patient was placed in the left lateral decubitus position for the planned video-assisted thoracoscopic surgery (VATS), and DLT positioning was again confirmed with fiberoptic bronchoscopy.
General anesthesia was maintained with balanced anesthesia using oxygen-air-sevoflurane (1-2 vol%) and continuous infusion of remifentanil. After endotracheal intubation, 40 mg of rocuronium was administered and an additional dose of 10 mg was administered twice until the event described below occurred. Mechanical ventilation during OLV was initiated using pressure-controlled ventilation-volume guaranteed mode with a tidal volume of 300 ml and a respiratory rate of 14 breaths/min. After about 30 min of procedure, VATS was converted to thoracotomy due to surgical site adhesion. Peak airway pressure (PAP) was 14 cmH2O during two-lung ventilation. After OLV, the PAP was 25 cmH2O initially and gradually increased to 35 cmH2O within 10 min. SpO2 gradually decreased from 97% to 80% during the next 5 min. As a rescue measure, two-lung ventilation was performed for several minutes and SpO2 increased to 96%. After reapplication of the OLV, SpO2 gradually decreased from 98% to 70%. Inspired oxygen was increased from 60% to 100%, and two lung ventilation was reinstituted. Oxygen saturation increased to 95% for approximately 5 min. Systolic blood pressure decreased to 70 mmHg; subsequently, 100 µg of phenylephrine was administered twice and infused continuously. However, blood pressure was maintained as 85/60 mmHg. The ABGA (FiO2 1.0, EtCO2 23 mmHg) was checked and the outcomes were pH 7.223, PaCO2 60.9 mmHg, PaO2 61.9 mmHg, and SaO2 85.6%. Dopamine infusion (10 µg/kg/min) was started and systolic blood pressure was maintained above 100 mmHg. With intermittent suction of the DLT, oxygen insufflation into the non-dependent lung and dopamine administration, SpO2 was maintained between 85-90% during OLV. Subsequently, the PAP was noted to be about 35 cmH2O (maximum 37 cmH2O). We did not apply positive end-expiratory pressure to the dependent lung because of the high PAP. Nearly 2 h after the operation, systolic blood pressure suddenly dropped below 80 mmHg and fell below 50 mmHg within 1 min, SpO2 decreased from 90% to 70%, and EtCO2 decreased to 17-18 mmHg. Almost immediately, the arterial waveform disappeared and asystole was revealed on ECG. Two-lung ventilation was reinstituted and the surgical site was temporarily closed using dressing films. The patient was placed in the supine position and resuscitated with atropine and epinephrine, and the surgeon started closed cardiac compression. At the same time, we asked for help in applying ECMO. About 17 min later, recovery of spontaneous circulation achieved. Nearly at the same time, veno-arterial (VA) ECMO was also started via the right common femoral artery and common femoral vein. On auscultation, lung sound of the left lung field was decreased markedly. Tension pneumothorax of the dependent left lung was suspected. Portable chest X-ray revealed tension pneumothorax of the left lung (Fig. 2) and a chest tube was inserted immediately. Follow-up chest X-ray showed re-expansion of both the lungs (Fig. 3). The patient was returned to the left lateral decubitus position, and the right upper lobectomy was performed after the right lung was selectively collapsed. At this time, the left lung was ventilated with a tidal volume of 250 ml and a respiratory rate of 13 breaths/min, and PAP was about 35 cmH2O. After completion of the surgical procedure, the DLT was replaced with a single lumen endotracheal tube of 7.5 mm internal diameter, and the patient was hemodynamically stable. He was transferred to the intensive care unit while maintaining VA-ECMO.
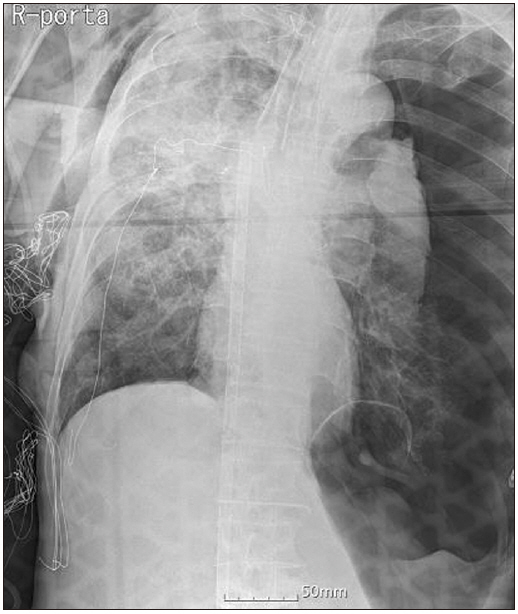
Fig. 3
Chest anteroposterior immediately after insertion of the chest tube shows re-expansion of the left lung.

Immediate postoperative echocardiography revealed moderate LV global and severe right ventricle (RV) free wall motion abnormality and decreased LV systolic function (EF = 40%). On the 10th day, transthoracic echocardiography showed normal LV global wall motion but still severe RV free wall motion abnormality was apparant. On the 14th day, echocardiography revealed normal RV free wall motion. Finally, ECMO was weaned off and the patient’s trachea was extubated.
DISCUSSION
Tension pneumothorax is an uncommon condition that can be fatal if left untreated [2]. Intraoperative tension pneumothorax can be extremely dangerous, especially during OLV and is a rare complication. It can cause sudden death or serious long-term organ damage. There exist a few case reports in the literature on contralateral tension pneumothorax during OLV in recent decades. Hoechter et al. [3] reported that there were only 9 cases published in the literature so far in 2018. However, the authors reported pneumothoraces in 4 of 2,494 patients who underwent OLV for 5.5 years and mentioned the possibility of underreporting.
Clinical manifestations of tension pneumothorax include an immediate and progressive decrease in SpO2, immediate reduction in cardiac output, increase in airway pressure, ventilatory disturbances of the ipsilateral lung, venous distension, and loss of breathing sounds on the affected side in patients undergoing mechanical ventilation [1,4-8]. These clinical findings are caused by shifting or compression of mediastinal structures and the lung parenchyma, or the presence of air in anatomic spaces. Decreased cardiac output is probably due to a combination of hypoxemia, reduced venous return, and compression of great the vessel, ventricle, and opposite lung [5]. If the pneumothorax is not recognized and treated urgently, the condition might lead to sudden cardiac arrest [1]. In the present case, cardiac arrest occurred within 3 minutes of the drop in blood pressure. These signs may not be apparent if the opposite chest is open during a surgical procedure, because mediastinal shift may not compress these structures to the extent when the chest is closed [5]. Finlayson et al. [4] reported a case of a patient with contralateral tension pneumothorax during thoracotomy without typical signs of marked hypoxemia and hemodynamic instability. The patient may show clinical manifestations only after the chest is closed [5]. In some cases, patients can show increased airway pressure and decreased oxygen saturation with only transient hypotension [9]. Therefore, even in the absence of typical signs such as hypoxemia and hypotension, the possibility of tension pneumothorax should not be overlooked in any patient who develops high peak inspiratory pressures during OLV with an open chest [4]. However, in the present case, the left tension pneumothorax prevented adequate venous return, even when the right chest was opened, resulting in complete cardiovascular collapse, as also reported by other authors [6,7,10,11]. Finlayson et al. [4] reported that in half of the cases, the cardiovascular collapse occurred before decompression of the pneumothorax.
Diagnosis is often delayed because the classic signs of tension pneumothorax are similar to the common clinical manifestations during OLV. Other causes such as DLT malposition, bronchial occlusion by secretions or blood, and dynamic hyperinflation of the lung are usually considered first [4]. In addition, the lateral decubitus position and surgical drapes make access to the dependent hemithorax for physical examination difficult. Checking the collapsed bronchus with a fiberoptic bronchoscopy can also help with diagnosis [9,12] before confirming tension pneumothorax with chest radiography. In the present case, two-lung ventilation was resumed because of the possibility of tension pneumothorax, but cardiac arrest occurred quickly. Consequently, we started cardiopulmonary resuscitation after placing the patient in a supine position and asked the ECMO team for help. There exist a report which states that mediastinal thoracentesis was carried out without a definite diagnosis in nearly fatal case, as diagnostic methods took time and there was no time to delay the treatment [13]. However, in most of the cases, a diagnostic method such as chest X-ray or ultrasound is used to identify pneumothorax before attempting decompression.
In the present case, barotraumas is hypothesized as the possible cause of tension pneumothorax and it may occur as a result of air trapping within the dependent lung, leading to hyperinflation and rupture of bulla [12]. In previous case reports on tension pneumothorax during OLV, many cases were associated with barotraumas [3-7,10-14]. Some of them were related to inappropriate DLT size [7,10,12], and some were related to rupture of bulla [12,13]. Sometimes patients undergoing lung surgery have pre-existing pulmonary conditions such as emphysema or bulla. In the diseased lungs, reduction in elasticity and compliance occur and the high ventilation pressures can affect the vulnerable lungs and lead to pneumothorax [3]. In patients with chronic obstructive lung disease and pulmonary hyperinflation, intrinsic positive end-expiratory pressure is common during OLV, which can lead to an excessive increase in airway pressure and decrease in tidal volume during OLV [15]. In this case, the patient had COPD accompanied by emphysema with bullae in bilateral lungs. Therefore, our patient had a risk of pneumothorax. Use of recruitment maneuvering techniques at high pressures can cause pneumothorax with barotraumas [4,5].
In conclusion, contralateral pneumothorax during OLV is rare but can occur at any time. It may be associated with sudden death or serious long-term complications. Hoechter et al. [3] noted that only four out of the nine previously reported cases led to a correct diagnosis with clinical suspicion. Therefore, anesthesiologists should consider, be alert, and cope with this rare but critical complication.




