INTRODUCTION
Selective transforaminal epidural block (STE) has come to the fore as a target-specific modality in the treatment and diagnosis of spinal pain [
1-
3]. STE may provide considerable effect at a desired location with a small dose of drug, as the technique involves placement of a needle into the intervertebral foramen, from which the nerve originates, and injection of the drug into the anterior part of the epidural space and the surrounding portion of the nerve root [
4,
5]. However, STE should be performed with care because it may result in complications such as intravascular injection, air embolism, vascular injury, cerebral embolism, epidural hematoma, and spinal cord injury [
6].
Thoracic transforaminal epidural block (TTFEB), which is performed for the treatment of pain at the level of the thoracic vertebrae, should be carried out with special care because TTFEB has the associated risk of pneumothorax, in contrast to STE performed at the cervical or lumbar vertebrae. In addition, TTFEB requires caution because of the technical complications and the anatomical structure of the epidural space, which is narrow and close to the spinal cord [
7,
8]. In the conventional TTFEB method, a line parallel with the vertebrae is drawn from a point externally separated by 40 mm from the spinous processes, and the intersection point of the line with the inferior margin of a target vertebral body or with the extension line thereof is determined under fluoroscopy as the needle entrance point [
9]. This approach is used because there is a risk of pneumothorax if the needle is passed or inserted to lateral part of the line. In most cases, TTFEB is performed by the conventional method [
9], this is a standard that does not take into account the individual shape of each patients. Therefore, to perform TTFEB safely without complications in Koreans, especially elderly Korean individuals, who tend to have smaller body types with the physical characteristics of Asians, there is a need to investigate the TTFEB angle and method appropriate for Koreans.
This article describes a retrospective study conducted using computed tomography (CT) imaging to investigate the TTFEB angle and depth appropriate to minimize the risk of pneumothorax in Koreans.
MATERIALS AND METHODS
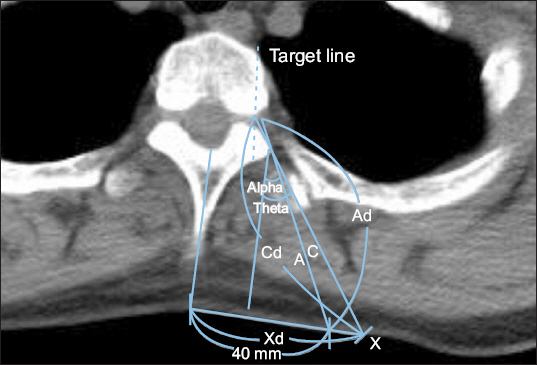
The subjects of the present study were 100 randomly selected patients between 50 and 70 years of age found be free of thoracic disease according to chest CT performed in the present hospital. On the chest CT, the superior, middle, and inferior thoracic vertebrae were observed at the T2, T7, and T11 levels, respectively. The selected chest CT imaging plane allowed straight access from the inferior part of the vertebral body column to the intervertebral foramen (
Fig. 1). Firstly, the needle insertion distance (Ad) and angle (alpha) were measured along the line drawn from a point 40 mm external from the spinous process, grazing the exterior margin of the lamina and arriving at the 1/2 depth of the intervertebral foramen, according to the conventional method. At this time, if the needle tip is located inside the pedicle’s midline, the risk of dural puncture increases, so the midline of the pedicle on the CT is set as the target point of the needle. However, when the needle is inserted at the 40 mm point, it may be difficult to reach the target point depending on the patient’s body shape. Therefore, we studied the experimental TTFEB angle and distance for measurement of the angle appropriate for the body shape of Koreans. To determine the minimum angle at which to reach the target point in 1/2 depth of intervertebral foramen without causing lung injury, the point where the line from the 1/2 depth of the intervertebral foramen meets the skin at the minimum angle possible without intersecting the lung was determined as Point X in the T2, T7, and T11 CT images (
Fig. 1). Then, the distance from the needle insertion point (X) to the spinous process (Xd), the needle insertion depth to the 1/2 depth of the intervertebral foramen (Cd), and the needle insertion angle (theta) were measured.
Fig. 1
Computed tomography images and measurement values. Ad: needle insertion distance along the line drawn from the point 40 mm external from the spinous process, grazing the exterior margin of the lamina and arriving at the 1/2 depth of the intervertebral foramen, Alpha: needle insertion angle along the line drawn from the point 40 mm external from the spinous process, grazing the exterior margin of the lamina and arriving at the 1/2 depth of the intervertebral foramen, Cd: needle insertion distance along the line drawn from Point X, grazing the exterior margin of the lamina and arriving at the 1/2 depth of the intervertebral foramen, Theta: needle insertion angle along the line drawn from Point X, grazing the exterior margin of the lamina and arriving at the 1/2 depth of the intervertebral foramen, Xd: distance from Point X to the spinous process, X: needle insertion point where the line form the 1/2 depth of the intervertebral foramen contacts the skin without passing through the lung at the minimum angle.
To determine the maximum angle at which to perform TTFEB without causing lung injury, the point where the line from the 1/2 depth of the intervertebral foramen meets the skin at the greatest angle possible without intersecting the lung was determined as Point Y in the T2, T7, and T11 CT images (
Fig. 2). Then, the distance from Point Y to the 1/2 depth of the intervertebral foramen was measured with the needle insertion depth (Dd) and the maximum angle (delta). In addition, the distance from the spinous process to the needle insertion point, Point Y (Yd) was measured.
Fig. 2
Measurements on computed tomography images at T11 level. Dd: needle insertion distance along the line drawn from Point Y to the 1/2 depth of the intervertebral foramen without passing through the lung, Delta: needle insertion angle along the line drawn from Point Y to the 1/2 depth of the intervertebral foramen without passing through the lung, Yd: distance from Point Y to the spinous process, Y: needle insertion point where the line from the 1/2 depth of the intervertebral foramen contacts the skin without passing through the lung at the largest angle.

The average, standard deviation, minimum, and maximum were calculated for each of the values, and a multiple regression analysis was performed to investigate the correlation between the variables.
DISCUSSION
Epidural block is performed for control of spinal pain. Although STE entails a complicated procedure and involves radiation exposure, STE provides a greater effect on a desired part with a small dose of drug in comparison to the conventional interlaminar approach, because the drug may be injected at the nerve root and the anterior meningeal epidural space associated with a lesion [
10,
11]. In principle, STE may be performed at the cervical, thoracic, and lumbar vertebrae, and demonstrates a powerful effect in the control of radiating pain, particularly at the lumbar vertebrae. Therefore, STE has been performed extensively [
12,
13].
However, STE may lead to various complications such as dural puncture, spinal cord injury, infection, hematoma, abscess, subdural injection, intracranial air injection, pneumothorax, nerve injury, headache, cerebral injury, intracranial hypertension, intravascular injection, and vascular injury [
1,
5]. Efforts have been made to perform the procedure safely with prevention of complications. For accurate placement of the needle, the procedure is usually performed under fluoroscopy, despite the radiation exposure. Fluoroscopy enables a surgeon to inject the drug to the desired location while viewing the spread of the contrast agent, but complications may not be completely prevented.
Some of the possible complications result from the anatomical structure of the operated part. The cervical vertebrae have a complicated blood supply structure in comparison to other parts, and thus the incidence rate of intravascular injection is high. Therefore, there is a high possibility of spinal cord infarction with such complications as convulsions, coma, and death, requiring special cautions [
14,
15]. The radiculomedullary artery (artery of Adamkiewicz) is vulnerable to external injury by the needle for nerve block [
16]. The artery of Adamkiewicz enters the spinal canal from either the thoracic vertebrae or the lumbar vertebrae, but is vulnerable at the superior part of the left lumbar or the inferior part of the thoracic spine [
17]. According to Murthy et al. [
17], about 97% of the artery of Adamkiewicz passes through the safe triangle under the pedicle. Owing to this anatomy, insertion of the needle aimed at the conventional safe triangle may cause severe complications between T9-L3, where the artery of Adamkiewicz is most frequently located [
18]. Hence, the needle should be aimed at Kambin’s triangle, and the retrodiscal approach, which has been used as an adjuvant method of TTFEB, is preferred in that region [
16,
19].
Pneumothorax refers to the abnormal presence of air in the space between the visceral pleura and the parietal pleura and may be caused spontaneously or by direct or indirect trauma [
20]. The incidence rate of iatrogenic pneumothorax, caused by diagnostic and therapeutic actions, has recently increased, as invasive diagnostic tests and other procedures are performed with greater frequency. TTFEB may increase the incidence rate of pneumothorax depending on the needle position or the needle insertion point. A patient with pneumothorax reports such symptoms as chest pain or respiratory distress. The symptoms of pneumothorax are generally observed immediately after the procedure but may appear as much as 24 hours later in rare cases [
21]. Horner’s syndrome may occur in rare cases, as the stellate ganglion is pulled by the movement of the mediastinum owing to pneumothorax [
22], resulting in physical distress for the patient as well as mental distress for both the patient and the medical staff. Therefore, an accurate operative method and precautions are required to prevent complications.
Although the thoracic vertebra has a wide and long lamina and a transverse process with a wide base, the intervertebral foramen is difficult to reach. While selective nerve root block may be performed at T11 and T12 as in the lumbar vertebra, an appropriate image is difficult to obtain owing to the costa, which may be an obstacle to movement of the needle in TTFEB. Therefore, a needle with a slightly bent tip is more useful than a straight needle [
23]. Even though the costa may be an obstacle to needle movement during the procedure, it protects the structures in the posteromedial part of the mediastinum and guides the needle toward the intervertebral foramen [
23].
In the conventional TTFEB method, a line parallel with the vertebra is drawn from a point externally separated by 40 mm from the spinous process, and the intersection point of the line with the inferior margin of a target vertebral body or with the extension line thereof is determined under fluoroscopy as the needle entrance point [
9]. According to the results of the present study, when TTFEB is performed at the point externally separated by 40 mm from the spinous process, the needle insertion angle was 17.7 ± 4.3°, 27.6 ± 4.1°, and 24.2 ± 4.5° at T2, T7, and T11, respectively. The needle insertion angle at T2 was significantly smaller than that at T7 and T11, most likely because the anatomical structure of the lamina of the T2 vertebral body [
24] is different and the insertion distance at T2 is significantly longer needle than that at T7 and T11. For this reason, the average distance from the needle insertion point (X), where the line from the external boundary of the vertebral body in parallel with the line drawn by the conventional method (A) meets the skin (B), to the intervertebral foramen (Xd, T2: 62.9 ± 12.6 mm, T7: 48.2 ± 9.3 mm, and T11: 42.8 ± 10.9 mm) may have been found to be significantly longer at the T2 level.
In addition, needle insertion along the line from the needle insertion point (X) through the thoracic lamina into the thoracic intervertebral foramen (C) did not damage the lung. The distance from the spinous process to the needle insertion point (X) measured at T2, T7, and T11 was 62.9 ± 12.6 mm, 48.2 ± 9.3 mm, and 42.8 ± 10.9 mm, respectively, longer than the distance of 40 mm in the conventional method. The needle insertion angles measured at T2, T7, and T11 were 32.8 ± 7.4°, 35.1 ± 7.4°, and 26.1 ± 11.2°, greater than the angle in the conventional method, in which the needle is inserted at a point 40 mm away from the spinous process.
As the results of the present study demonstrate, the needle may be inserted from a position that is separated from the spinous process by more than 40 mm, according to the measurements of the present experiment, while the aim of the needle remains within the external boundary of the vertebral body and grazes the exterior margin of the lamina. This approach can cause more pain because of the longer distance, but may enable the needle tip to enter further into the intervertebral foramen, helping the surgeon to perform the nerve block more successfully. However, the distance from the needle insertion point (X) to the spinous process measured at T2, T7, and T11 was 62.9 ± 12.6 mm, 48.2 ± 9.3 mm, and 42.8 ± 10.9 mm, respectively, indicating that the distance decreased as the level was lowered.
The theoretically longest distance that allows implementation of TTFEB without causing lung injury at T2, T7, and T11 is 98.8 ± 10.2 mm, 90.7 ± 10.1 mm, and 98.8 ± 10.2 mm, respectively. Therefore, TTFEB may be performed from a point farther from the spinous process. In such cases, however, the needle insertion angle should be very large, specifically 58.1 ± 6.1°, 61.7 ± 4.3°, and 64.4 ± 7.0°, respectively, and a slight external alteration of the needle direction from the direction to the exterior margin of the lamina may drastically increase the risk of the injury to the lung. Therefore, when performing TTFEB in actual clinical practice, it is probably it is probably safe to refer to the measured value at Point X.
The results of statistical analysis showed that the needle insertion distance to the intervertebral foramen and needle insertion angle were increased in TTFEB as the weight of the subjects increased. This correlation may be applied in clinical settings to vary the needle insertion distance and angle depending on a patient’s weight to perform TTFEB more safely.
In the present study, measurements were performed using chest CT images, which may differ from the cross-sections for needle insertion in actual TTFEB procedures. This may be a limitation of the present study. TTFEB should be conducted carefully in patients with advanced age, degenerative intervertebral disc disease, history of spinal surgery, and alteration of the joint, because anatomical deformation may be caused by the procedure [
25].
The need for STE in spinal pain control is increasing, and numerous studies have been conducted regarding the effects of STE. However, as the possible complications of STE may be fatal, painstaking efforts should be made to perform STE safely. The present study was conducted to investigate the appropriate needle insertion distance and angle in the performance of TTFEB in Korean patients. The results of the present study may be used as a reference for a safe procedure rather than an absolute standard. In addition, further study may be required regarding variation in measurements among individual patients.







