제왕절개술을 위한 척추마취 동안 저혈압 예방을 위한 phenylephrine 부하용량의 효과
The effects of a loading dose of phenylephrine for the prevention of maternal hypotension under spinal anesthesia for Cesarean section
Article information

Abstract
Background:
Phenylephrine is frequently used for the prevention and treatment of maternal hypotension in patients undergoing Cesarean section. But there are limited studies about the prophylactic effect on maternal hypotension with a loading dose, followed by a continuous infusion of phenylephrine. Therefore, we investigated the additional effect of a loading dose infusion of phenylephrine on the prevention of maternal hypotension, and compared it to a continuous infusion of phenylephrine without a loading dose.
Methods:
Following spinal anesthesia, sixty-four patients were randomly assigned to one of two groups according to the phenylephrine administration regimen: group L (n = 32; loading dose [200 μg/min] just before continuous infusion [20 μg/min]) and group C (n = 32; continuous infusion [20 μg/min] without a loading dose). We measured the blood pressure and heart rate, and assessed the incidence of hypotension, nausea, vomiting, dosage of used rescue drugs and fetal parameters.
Results:
At 2, 4 minutes after administration of phenylephrine, group L showed a higher systolic blood pressure and lower heart rate than group C. However, there were no significant differences in the incidence of hypotension, nausea, vomiting and the dosage of used rescue drugs. There were no significant differences in the fetal parameters such as Apgar scores and umbilical pH.
Conclusions:
The loading dose infusion of phenylephrine had no beneficial positive effect on the prevention of maternal hypotension.
서론
제왕절개술을 위한 척추마취는 마취의 발현이 빠르고 차단이 확실하게 되며 실패율도 낮기 때문에 많이 사용되는 부위마취 방법이지만, 교감신경 차단효과에 의해 저혈압이 발생할 수 있으며, 이로 인해 자궁태반관류(utero-placental circulation) 장애로 태아 저산소증 등의 합병증이 발생할 수 있다. 그러므로 척추마취로 인한 산모의 저혈압을 예방 및 치료하기 위해 수액 전부하 및 승압제 사용이 추천되고 있으며 승압제로 ephedrine과 phenylephrine이 사용되고 있지만, 태아의 산-염기 균형을 더 잘 유지시키는 phenylephrine이 최근 더 선호되고 있다[1]. 이에 따라 phenylephrine의 적정 투여 용량 및 용법에 대한 연구가 정주 방법 및 용량에 따라 세분화되어 이루어지고 있으나[2–4] 최적의 투여 요법에 대한 확립이 되어 있지는 않다. 초기 연구에서는 20–40 μg phenylephrine 저용량 일시 주입 방법이 저혈압 예방 효과가 있다는 결과가 있었으나[3,5] 점차 phenylephrine의 고유량 정주 또는 지속 주입에 대한 연구가 이루어지고 있다[2,6].
그래서 저자들은 산모에게 예방적으로 phenylephrine 부하용량 사용군과 부하용량 없는 지속 정주군으로 나누어 주입함으로써 phenylephrine 정주 방법의 차이가 산모와 태아에 미치는 영향을 알아보고자 본 연구를 계획하였다.
대상 및 방법
본 연구는 미국마취과학회(American Society of Anesthesiologists) 신체등급분류(American Society of Anesthesiologists physical status classification) II에 해당하는 건강한 만삭의 산모 중에서 척추마취에 의한 제왕절개술이 계획된 산모 70명을 대상으로 하였으며 본원 임상연구심의위원회의 승인 및 환자의 동의를 얻은 후 진행되었다. 자간전증/자간증을 포함한 심혈관계, 뇌혈관질환이 있는 산모와 산전 검사상 다태아나 기형아인 경우, 부위마취의 금기증이 있거나 환자가 거부하는 경우 그리고 산모의 초기 수축기 혈압이 100 mmHg 미만인 경우는 제외하였다.
마취 전 투약은 실시하지 않았고 수술 전 한쪽 팔에 18 G 정맥도관을 거치하여 정질액 500 ml와 교질액 250 ml를 척추마취 시행 시 주입하였으며, 앙와위 자세에서 심전도, 맥박산소포화도 계측기와 비침습적 자동 혈압기를 부착하여 기저치로 기록하였다. 앉은 자세에서 척추마취를 시행하여 척수강 내 0.5% bupivacaine 9–10 mg과 fentanyl 20 μg을 주입하여 피부분절(cold sensory block level) T4까지 감각 차단하는 것을 목표로 마취를 시행하였다. 마취 후 앙와위 자세를 취하고 오른쪽 둔부 아래 쐐기(right lumbar wedge)를 적용한 후 비침습적 자동 혈압기를 사용하여 혈압을 측정하였다. 기준 혈압(baseline blood pressure)은 연속 3회 측정하여 그 평균값을 취하고 기준 심박수(baseline heart rate)도 동일한 방법으로 측정하였으며 그 후 2분 간격으로 혈압, 심박수를 측정하여 기록하였다. 연구에서 사용된 phenylephrine (phenylephrine Hcl, Hana Pharmaceuticals, Korea)은 생리식염수와 혼합하여 희석된 약제(100 μg/ml)로 두 군에서 사용하였다.
대상 환자는 무작위 두 군으로 배정하였으며, 척추마취 시행 직후에 혈압 강하 예방 목적으로 phenylephrine 부하용량(loading dose)을 정주한 후 지속 정주한 군(Group L)과 부하용량 없는 지속 정주군(Group C)으로 나누어 산모의 혈역학적 지표와 신생아에 미치는 영향을 분석하였다. Group L은 phenylephrine 200 μg/min을 1분 동안(120 ml/h) 부하용량을 정주한 다음 20 μg/min (12 ml/h)을 마취시간 동안 지속 주입하였고 Group C는 부하용량 없이 20 μg/min (12 ml/h)을 지속 주입하였다. 두 군 모두에서 20 μg/min 지속 정주는 20분 동안 시행 후 중단하였다. 마취 유도 전과 비교하여 수축기 혈압이 20% 이상 감소하였거나 100 mmHg 미만으로 감소하였을 경우 phenylephrine 100 μg을 정주하였으며, 저혈압이 지속되면 효과가 나타날 때까지 phenylephrine 25 μg을 매분 주입하였다. 반대로 수축기 혈압이 기준값과 비교하여 20% 이상 증가하면 phenylephrine의 주입을 중단하였다. 또한, 마취 유도 중 심박수가 50회/분 이하일 경우는 atropine 0.5 mg을 정주하고, 저혈압과 서맥이 동반되었을 경우는 ephedrine 5 mg을 정주하였다. 수술 시간이 신생아 상태에 미치는 영향을 알아보기 위해 피부절개-분만시간(skin incision-delivery time, SDT), 자궁절개-분만시간(uterine incision-delivery time, UDT), 척수강주사뼷龜맒챨–(intrathecal injection-delivery time, IDT)을 기록하였고, 저혈압, 고혈압, 서맥, 오심과 구토의 빈도를 확인하였다. 수술 종료 후 의무기록을 확인하여 신생아의 Apgar score 1, 5분 점수와 제대동맥 가스분석을 기록하였다.
이전에 시행한 pilot study에서 phenylephrine을 부하용량 정주한 군(Group L)의 수축기 혈압 평균과 표준편차는 136.9 ± 20.5 mmHg, 부하용량 없이 지속 주입한 군(Group C)의 평균과 표준편차는 120.2 ± 25.6 mmHg로 나타났다. G power로 계산한 결과, effect size 0.7188372가 나왔고, alpha error = 0.05, power = 0.80로 설정하였을 때 표본 수는 각각 32명으로 계산되었고 10% 탈락률을 적용하여 총 70명을 대상으로 하였다. 모든 자료의 결과는 평균 ± 표준편차로 표시하였다. 나이, 신장, 체중, 제태기간, 피부분절 T6까지 이른 시간, 사용된 마취약제의 총량, 두 군 간의 시간에 따른 수축기 혈압과 심박수, 신생아의 Apgar score, 제대동맥 pH는 unpaired t-test를 이용하였으며, 비모수 지수에 대해 chi-square test를 이용하여 비교하였다. 통계분석은 SPSS (version 12.0, SPSS Inc., USA)를 이용하였으며 P값이 0.05 미만인 경우를 통계적으로 유의한 것으로 간주하였다.
결과
본 연구는 group L과 group C 각각 35명을 대상으로 하였으나 70명의 환자 중 2명은 척추마취를 실패하여 전신마취를 시행하였으며, 4명의 환자는 참가를 거절하여 두 군은 각각 32명을 대상으로 하였다(Fig. 1). 두 군 간의 나이, 키, 몸무게, 제태기간, bupivacaine 사용량의 통계적 차이는 없었으며 최대 감각 차단의 범위 및 T6 높이까지 이르는 시간도 유의한 차이가 없었다(Tables 1 and 2). 피부절개-분만시간(SDT), 자궁절개-분만시간(UDT), 척수강주사-분만시간(IDT) 모두 통계적 차이가 없었다(Table 2).

Flow diagram of the patients. Sixty-four patients were randomized for the study. Group L: loading dose (200 μg/min) of phenylephrine followed by a continuous infusion (20 μg/min), Group C: continuous infusion of phenylephrine without a loading dose.

Patients Characteristics

Anesthetic and Operative Data
Apgar score 1분, 5분, 신생아의 체중, umbilical arterial blood gas analysis 상 두 군 간의 유의한 차이가 없어 phenylephrine의 투여 방법에 따라 태아에게 미치는 영향의 차이는 없는 것으로 나타났다(Table 3).

Newborns’ Characteristics
척추마취를 시행하고 2분, 4분 후 group L의 수축기 혈압은 각각 136.6 ± 19.3 mmHg, 133.5 ± 20.3 mmHg로 119.9 ± 25.2 mmHg, 122.5 ± 22.3 mmHg로 측정된 group C에 비하여 유의하게 높았다. 상대적으로 2분에서 심박수는 group L에서 group C에 비해 유의하게 낮았으며(72.3 ± 19.2 beats/min vs. 88.5 ± 18.5 beats/min, P = 0.001), 4분에서도 group L에서 유의하게 낮게 측정되었다(73.2 ± 19.4 beats/min vs. 83.4 ± 20.0 beats/min, P = 0.043). 고혈압과 서맥의 빈도는 통계적으로 유의한 차이는 없었다(Fig. 2, Table 4).
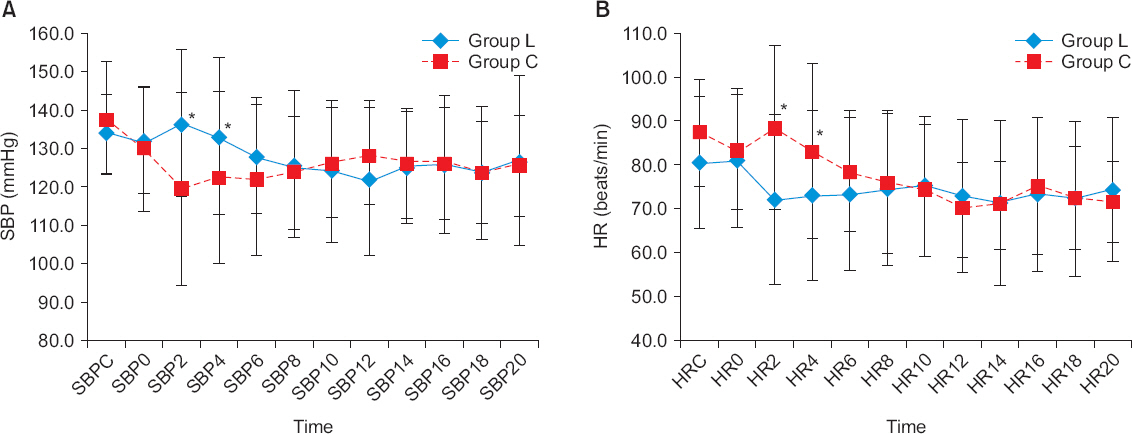
Changes of (A) systolic blood pressure (SBP) and (B) heart rate (HR) of perianesthetic period. Values are expressed as mean ± SD. Group L: loading dose (200 μg/min) of phenylephrine followed by a continuous infusion (20 μg/min), Group C: continuous infusion of phenylephrine without a loading dose. SBPC: SBP before phenylephrine infusion, SBP0–20: SBP at 0–20 minutes after phenylephrine infusion. HRC: HR before phenylephrine infusion, HR0–20: HR at 0–20 minutes after phenylephrine infusion. *P < 0.05 between two groups.

The Prevalence of Adverse Events and Doses of Rescue Drugs
고찰
제왕절개를 위한 부위마취를 시행할 때 교감신경계 차단에 의한 혈관 확장 효과로 발생하는 저혈압이 산모와 태아에 악영향을 미칠 수 있다. 자궁의 혈류량은 산모의 혈압에 직접적인 영향을 받으며, 자동조절기능이 없어서 저혈압이 발생했을 때 혈압에 비례하여 자궁 혈류량이 감소하게 되는데, 이에 따라 태아의 산소공급이 저하되고, 산증이 유발되어 합병증이 발생할 수 있다[7,8]. 따라서 제왕절개를 위해 마취를 시행하고, 유지하는 동안 산모의 혈역학적 안정을 유지하는 것이 산모와 태아 모두에게 안전하고 적절한 마취를 제공하는 것이다.
Prophylactic phenylephrine과 placebo를 비교한 선행의 연구들에서 phenylephrine은 분만 전의 저혈압을 감소시킨다는 결과(relative risk, 0.36; P = 0.004)를 보여 최근에는 제왕절개 시 부위마취 후에 나타나는 저혈압의 치료에 많이 사용되고 있다[9-11]. Phenylephrine을 사용할 경우 산모의 서맥, 고혈압, 오심과 구토 같은 부작용의 발생빈도 역시 대조군과 비교했을 때 유의하게 증가되지 않는다는 연구도 있다[12,13]. 또한, das Neves 등[10]은 phenylephrine을 지속 정주하거나 일시 정주했을 때 1분 Apgar score가 증가된다는 보고를 하기도 하였으나 phenylephrine에 따른 Apgar score의 차이가 없다는 연구결과들도 있다[14]. 상반된 결과에도 불구하고 대부분의 연구에서 phenylephrine은 저혈압을 예방하는 데 효과적이며[6,15], ephedrine에 비하여 태아 제대정맥의 pH를 증가시키고, PCO2를 감소시켜 산염기 균형을 개선시킨다고 알려져 있다[16]. 그러나 phenylephrine의 최적의 투여 요법에 대해서는 확립이 되어있지 않다.
초기 연구에서는 20–40 μg phenylephrine 저용량 일시 주입 방법이 저혈압 예방 효과가 있다는 결과가 있었으나 점차 phenylephrine의 고유량 정주 또는 지속 주입에 대한 연구가 이루어지고 있다. Liu 등[17]은 0.5% bupivacaine 10 mg을 척추강 내로 단독 투여하고, 저혈압 발생을 억제하는 90% effective dose (ED90)를 알기 위해 phenylephrine을 60, 80, 100, 120, 140 그리고 160 μg을 continual reassessment method로 주입하였다. 위의 연구에 의하면 산모의 저혈압을 예방하기 위해 phenylephrine 일시 주입의 ED90는 100 μg 이었다. 또 다른 연구에서는 up-down sequential allocation method를 이용하여 ED90을 측정한 결과보다 높은 용량으로 150 μg으로 보고하기도 하였다[2]. 또한, Ngan Kee 등[9]은 3분 동안 100 μg/min을 주입하여 총 300 μg을 주입하였고, 추가로 수축기 혈압이 기준치보다 감소할 때마다 100 μg/min을 주입한 군과 수축기 혈압이 기준치의 80% 이하로 감소할 때마다 100 μg을 정주한 대조군을 비교한 결과 300 μg 이상을 투여한 군에서 대조군에 비해 저혈압의 빈도가 확연히 감소하였음을 보고하였다(6 [23%] of 26 vs. 21 [88%] of 24; P < 0.001). 이에 따라 본 연구에서는 대조군에 비하여 확연한 효과를 보인 300 μg과 ED90으로 측정된 100–150 μg의 중간값인 200 μg을 1분 동안 속도 조절 주입기(syringe pump)를 통하여 부하용량으로 정주를 시행하여 대조군과의 차이를 비교하였다. 저혈압의 발생이 척추마취 초기에 발생하기 때문에 본 연구에서는 1분 동안의 부하용량을 주입한 후 지속용량을 주입하는 것이 초기의 혈압저하 예방 효과가 우수할 것으로 판단하여 부하용량 정주를 실험군으로 설정하였다. Langesaeter 등[11]은 0.25 μg/kg/min의 저유량의 phenylephrine 주입을 통하여 대조군에 비해 유의한 저혈압 예방 효과를 보았으며, Allen 등[12]의 연구에서도 prophylactic phenylephrine 25–50 μg/min을 투여하여 산모의 혈역학 안정성을 확인하였다. 본 연구에서는 이들의 중간값인 20 μg/min으로 지속 주입 용량을 설정하였다. 이에 따라 phenylephrine 200 μg/min을 1분 동안 부하용량으로 정주한 다음, 20 μg/min의 속도로 지속 정주를 한 group L과 20 μg/min으로 부하용량 없이 지속정주를 한 group C로 나누어서 산모와 태아에게 미치는 영향을 조사하였다. 그러나 group L과 C 모두에서 태아에는 미치는 영향의 차이는 없었고, group L에서 phenylephrine 투여 2분과 4분에 group C에 비해 일시적으로 높은 수축기 혈압과 낮은 심박수를 보였다. 비록 고혈압 및 서맥 발생 빈도에서 유의한 차이를 보이지는 않았지만 부하용량 정주의 이득으로 기대했던 저혈압 예방 효과면에서 group C에 비해 탁월한 장점을 보이지 못하면서 고혈압과 서맥을 보이는 것은 group L의 한계로 생각된다. 이는 부하용량 없는 phenylephrine 지속 정주만으로도 저혈압 예방 효과가 있기 때문에 group L에서 초기에 과량의 phenylephrine의 투여가 저혈압 예방 효과의 장점보다는 과용량으로 인한 부작용으로 척추마취 후 2분과 4분에 일시적으로 고혈압과 서맥의 발생을 유발시킨 것으로 추정된다. 그러므로 본 연구 방법보다 phenylephrine 부하용량을 줄이고 부하용량 투여 시간을 늘리는 등의 새로운 접근을 통해 고혈압과 서맥 같은 부작용을 줄이면서 저혈압 발생을 억제할 수 있는 phenylephrine 사용 용량에 대한 후속 연구가 필요하리라 생각된다.
결론적으로 1분 동안 200 μg의 phenylephrine 부하용량 사용군(group L)이 부하용량 없는 지속 정주군(group C)에 비해 태아에게 미치는 영향과 저혈압 예방 효과는 비슷하면서 일시적으로 산모의 수축기 혈압을 증가시키고, 서맥을 발생시키므로 저혈압 예방 효과 측면에서 추가적인 장점이 없는 것으로 판단된다.
ACKNOWLEDGMENTS
This work was supported by the intramural research grant of Chungbuk National University in 2015.