Gastric distension and atelectasis after using a supraglottic airway - A case report -
Article information

Abstract
Background
Supraglottic airways (SGAs) are used during general anesthesia (GA) due to comfort. Certain complications are possible, such as gastric distension. The incidence of pulmonary aspiration of regurgitated gastric contents was found to be 0.02%. A difference in the incidence of gastric regurgitation was not identified between the use of SGAs and endotracheal intubation. We report a case of gastric distension and atelectasis in a patient in whom an I-gel® was used for GA.
Case
A 63-year-old female patient underwent triple arthrodesis on her ankle under GA using an SGA (I-gel® size 3). After surgery, she suffered from nausea and abdominal bloating. A chest radiograph revealed that a large amount of air in her stomach had caused gastric distention, which resulted in left hemidiaphragm elevation and atelectasis.
Conclusions
This case illustrates that the use of I-gel® in prolonged surgeries may result in malposition of the SGA and gastric insufflation and atelectasis.
Supraglottic airways (SGAs) are commonly employed in general anesthesia (GA) for enhanced patient comfort. Compared to endotracheal intubation, SGAs are less invasive with respect to the respiratory tract. In terms of hemodynamic stress, SGA placement and removal are less irritating to the patient than traditional airway-management techniques . Despite these advantages, anesthesiologists must also consider the risks before choosing an SGA. Specific complications can occur with the use of an SGA, such as gastric insufflation, mucosal damage, bleeding, dysphagia, and hoarseness, among others . We report the case of a patient who underwent orthopedic surgery under GA using an SGA, which resulted in gastric insufflation with left hemidiaphragm elevation and left lower-lobe atelectasis.
The incidence of pulmonary aspiration of regurgitated gastric contents when using SGA is known to be 0.02% . The incidence of pulmonary aspiration with endotracheal tube intubation is also comparable . The SGA cuff seal pressure is the pressure of inflation above which gas can escape around the cuff. This is lower than that achieved with a tracheal tube, so there is a greater risk of gastric insufflation, gastroesophageal reflux, and aspiration of regurgitated gastric contents when using an SGA . Devitt and colleagues studied gastroesophageal insufflation in 48 patients who received neuromuscular-blocking drugs and controlled ventilation through the SGA. Gastroesophageal insufflation occurred in only 2.1% of patients at an inflation pressure of 15 cmH2O but increased to 35.4% at that of 30 cmH2O .
We report a case of gastric distention in a patient who underwent orthopedic surgery under general anesthesia using an SGA, which eventually resulted in gastric insufflation and gastric distention. In this case, the patient’s gastric distention was so severe that she had left hemidiaphragm elevation and left lower-lobe atelectasis. This case report is unique in that gastric insufflation resulted in severe gastric distention and even left lower-lobe atelectasis.
CASE REPORT
A 63-year-old woman weighing 40 kg and measuring 160 cm tall presented with an American Society of Anesthesiologists physical status of III. She had previously been diagnosed with rheumatoid arthritis (RA), Sjögren’s disease, and bronchiectasis. The patient was scheduled for triple arthrodesis of the right ankle due to RA deformity.
As an RA patient, she did not have any immobility of neck motion and could extend her neck fully. Her Mallampati score was I, and her mouth-opening width was greater than three fingers between her upper and lower teeth. She had atlantoaxial subluxation on the c-spine extension flexion radiograph taken during pre-operational evaluation 1 day before the surgical procedure, and the atlanto-dens interval was about 4.2 mm.
She did not have a gastroesophageal reflux disease history or any other gastrointestinal problems that might have increased the possibility of gastric regurgitation. She completed 8 h of fasting before arriving to the operation room. She had no abnormal findings other than bronchiectasis on chest radiography (Fig. 1A) and a mild obstructive pattern on pulmonary function testing, which was part of her preoperative evaluation.
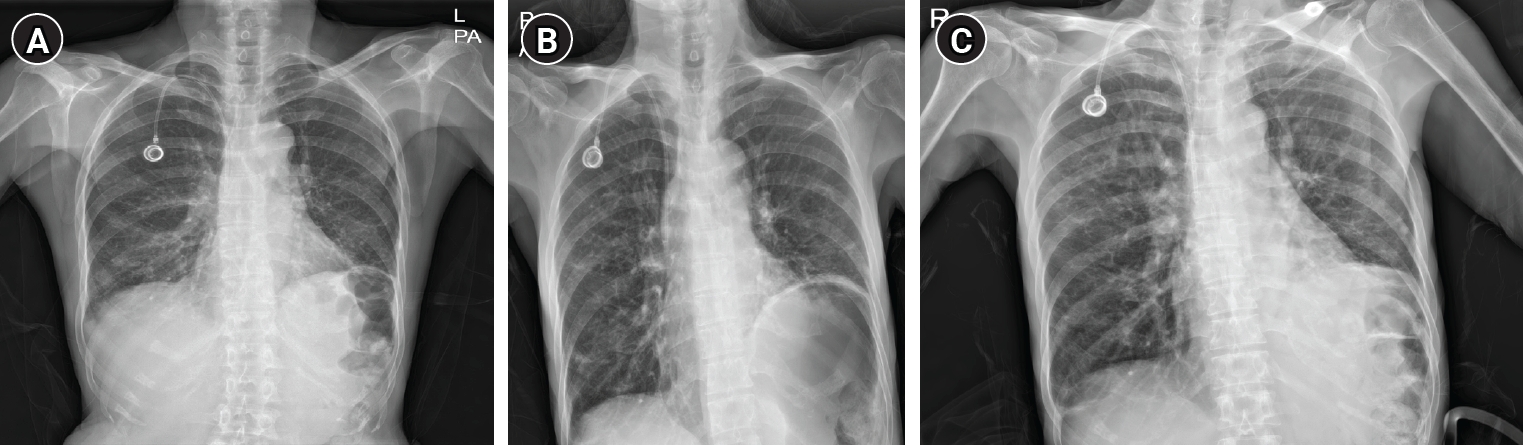
Chest radiographs. (A) A preoperative chest antero-posterior (AP) radiograph taken 2 weeks before surgery shows no abnormal findings other than bronchiectasis. (B) A postoperative chest AP radiograph image obtained a few hours after surgery shows gastric distension, left hemidiaphragm elevation, and left lower-lobe atelectasis. (C) A postoperative chest AP radiograph image taken 1 day after surgery shows left hemidiaphragm elevation.
Upon arrival to the operating room, her vital signs were as follows: heart rate, 70 bpm; blood pressure, 100/60 mmHg; and saturation of percutaneous oxygen (SpO2), 99% on room air. The patient coughed a lot and produced a significant amount of sputum, which she had to spit out just before induction, but her lung sounds were clear in both lungs. Induction of anesthesia was achieved with 50 mg of propofol and 0.1 mcg/kg/min of remifentanil delivered as a continuous infusion intravenously, and muscle relaxation was achieved with 30 mg of intravenous rocuronium under all standard American Society of Anesthesiologists monitoring protocols, including pulse oximetry, electrocardiography, non-invasive blood pressure monitoring, and temperature monitoring. After bag-mask ventilation for 3 min, a size 3 I-gel® (Intersurgical, Wokingham) was placed on the patient using the recommended insertion technique without any difficulty. There was no difficulty during the bag-mask process or insertion of the SGA. Placement of the SGA was confirmed by auscultation of breath sounds in both lungs and smooth capnograph tracing. The patient was mechanically ventilated using a volume-controlled ventilation mode (target tidal volume, 400 ml; I:E ratio, 1:2; fraction of inspired O2 concentration, 50%; and respiratory rate, 12 min). There was no mismatch between the patient’s actual tidal volume and the target tidal volume.
We used 2 vol% of sevoflurane to maintain one minimum alveolar concentration (MAC), and 0.05-0.1 mcg/kg/min of remifentanil delivered intravenously as a continuous infusion was used for the maintenance of anesthesia. The surgery lasted for a total of 4 h. The SedLine® electroencephalographic monitor (Masimo Corp.) was used to monitor the depth of anesthesia, and the value was maintained between 25-50. The patient was placed in the supine position throughout the surgery. Her peak airway pressure was maintained at approximately 15 cmH2O throughout the operation. Train-of-four (TOF) nerve stimulation was evaluated every 30 min and, when a TOF count of 4 was attained, 10 mg of rocuronium as a bolus was injected intravenously. After 60 min and then again at 130 min after anesthesia induction, 10 mg of rocuronium was delivered to the patient intravenously.
Ten min before the end of the surgery, the capnography showed a curare cleft; additionally, there was some air found to be leaking from the SGA, and the peak inspiratory pressure rose up to 30 cmH2O. An expiratory volume of only 350 ml was detected by the ventilator in contrast to the 400 ml inspirated tidal volume setting. The ventilator mode was changed to synchronized intermittent mandatory ventilation mode to avoid dyssynchrony between the patient’s spontaneous respiration and the ventilator. An up–down maneuver was performed to resolve the air leakage. The SGA was withdrawn by 5 cm, followed by reinsertion, and the difference between the inspiratory volume and detected expiratory volume was diminished. The patient’s residual neuromuscular blockade was reversed using 80 mg of sugammadex at the end of the surgery after confirming three twitches of TOF monitoring, and reversal was confirmed by all four twitches of TOF monitoring. After confirming that the patient's breathing and consciousness had recovered, the SGA was removed, and the patient was moved to the post-anesthesia care unit (PACU). In the PACU, the patient experienced mild symptoms of nausea and abdominal bloating, but these symptoms were alleviated at the time of discharge from the PACU without any medications. She did not have symptoms of dyspnea and breathed regularly at 12 times/min. SpO2 was maintained at 99-100% throughout her stay in the PACU. However, chest radiographs obtained 1 h after the discharge from the PACU confirmed gastric distension and consequent elevation of the left-side diaphragm and left lower lobar atelectasis (Fig. 1B) when compared to chest radiographs taken 2 weeks before surgery (Fig. 1A). The patient did not complain of any specific symptoms related to gastric distension, and the chest radiograph taken 1 day after surgery showed left hemidiaphragm elevation (Fig. 1C). The gastric distension disappeared, and the patient was discharged on the eighth postoperative day without any further complications.
DISCUSSION
Compared to endotracheal intubation, SGA has several advantages, and its use for airway-management purposes is increasing. In particular, it allows increased speed and reliability of placement by inexperienced personnel. For this reason, it is more convenient to use; thus, it can be adopted for the purpose of rescue airway management in difficult airway situations . In addition, there are many other advantages associated with SGA, such as the hemodynamic stability at induction and during emergence, the minimal changes in intraocular pressure, the low frequency of coughing during emergence, better oxygen saturation during emergence, and the low incidence of sore throat and voice alterations .
However, complications like gastric distension, gastric regurgitation, mucosal damage, bleeding, dysphagia, and hoarseness may occur with SGA use . Although there were no signs of SGA malpositioning at the time of insertion, this case included observations of severe gastric distension and atelectasis on the postoperative chest radiograph. This case can also be said to raise awareness of concerns when using SGA. As unrecognized gastric distension can result in gastric regurgitation and pulmonary aspiration, proper use of SGA as well as early recognition of and rapid response to possible complications are important clinical aspects.
Wahlen et al. [4] reported that SGA malpositioning was associated with a significantly increased incidence of gastric insufflation in children 3-11 years of age undergoing positive pressure ventilation, especially at an inspiratory airway pressure of > 17 cmH2O. In the publication by Latorre et al. [5], gastric air insufflation occurred in 19% (21/108) of patients; in 90.5% (19/21) of these patients, the SGA was malpositioned. Their study concluded that the incidence of gastric insufflation was associated with airway pressures of > 20 cmH2O and with clinically unrecognized SGA malpositioning in the hypopharynx. In that study, fiberoptic verification of the SGA position revealed suboptimal placement in 40% of cases. Thus, SGA malpositioning may occur frequently, which can lead to gastric insufflation.
Although the exact cause of gastric distension in our case remains unclear, several possibilities can be considered. First, it may have happened when air leakage occurred when the patient started breathing spontaneously 10 min before the end of the surgery. This leakage may have been caused by slight movement of the I-gel® during the spontaneous respiration of the patient. Second, the SGA may have been placed over the esophageal opening, causing gradual gastric distension due to positive pressure ventilation from the beginning of the surgery. According to a previous report, the longer an operation, the greater the amount of SGA movement that occurs over time, especially when the position of the SGA is not ideal . Although the position of the I-gel® was not initially confirmed using a fiberoptic bronchoscope at the beginning of the procedure, the inspiratory and expiratory volumes displayed by the ventilator remained relatively consistent throughout the surgery. Therefore, while this possibility is somewhat low, it cannot entirely be ruled out. Third, air may have been introduced during mask ventilation. Since gastric aspiration was not performed after SGA placement and the presence of gastric air was not confirmed by ultrasound, this explanation cannot be completely excluded. Fourth, it is possible that all or at least two of these possibilities occurred together. The patient produced a lot of sputum due to bronchiectasis, and these secretions cause airway resistance. There was a possibility that air could have moved into the stomach during mask ventilation or when the I-gel® shifted during the surgery.
Asai identified in their editorial four major factors that might increase the likelihood of regurgitation and aspiration, which are patient factors, operation factors, anesthesia factors, and device factors . The patient factors include a stomach that is not empty, which can be caused by several diseases and symptoms that delay gastric emptying, such as diabetes mellitus, increased intracranial pressure, hiatus hernia, gastrointestinal obstruction, recurrent regurgitation, and dyspeptic symptoms. Patients who have previously undergone upper gastrointestinal surgery, patients recently injured or receiving opioids, and women in labor also exhibit delayed gastric emptying. Morbidly obese patients and those with a volume of gastric acid that is > 25 ml with a pH of < 2.5 also have an increased risk of pulmonary aspiration. Among the operation factors, abdominal surgery and laparoscopic surgery lead to a greater risk of aspiration and lithotomy, and the head–down position may also encourage patients to regurgitate residual gastric contents . The incidence of regurgitation may be increased as the surgical time is extended. A shallow anesthesia depth may also increase the risk of aspiration, as airway reflexes (such as coughing, hiccoughs, or laryngospasm) or gastrointestinal motor responses (such as gagging or recurrent swallowing) may be evoked . Finally, patients receiving a classic laryngeal mask are at a higher risk of regurgitation and aspiration.
Fortunately, there were no long-term complications in our case, but gastric distension did occur after surgery. No matter how low the incidence, gastric distension carries a potential risk of gastric regurgitation, and gastric regurgitation can lead to potentially fatal consequences such as aspiration pneumonia. Therefore, efforts to prevent this are crucial. For this purpose, the selection of both SGA type and size is important, but correct positioning of the SGA is ultimately the most crucial aspect. Current methods to assess SGA placement include the following: auscultation, the leakage test, the bubble test, and fiberoptic examination . However, performing this in all patients may hinder the convenience of SGA. Therefore, it should be performed selectively in patients at risk of malposition or device failure, such as men, patients with impaired mandibular subluxation, patients with poor dentition, and older individuals . Ultrasound examination, which has the advantage of being non-invasive, simple, and reliable without a need to stop ventilation, can be an alternative. It has been reported that, similar to a fiberoptic examination, the ultrasound examination generally possesses comparable abilities in determining the position of the laryngeal mask airway . It can be used to minimize the need for fiberoptic instrumentation during airway manipulation through the device. Because gastric distension may occur at any time, periodic confirmation of position is necessary during a long surgery, and drainage of gastric juices through a drainage tube may be considered necessary to prevent complications.
Whatever the cause, gastric distension should always be treated cautiously due to the potential risk of gastric regurgitation. We report this case in hopes that it will be informative for surgeons who place SGAs.
Notes
FUNDING
None.
CONFLICTS OF INTEREST
No potential conflict of interest relevant to this article was reported.
DATA AVAILABILITY STATEMENT
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
AUTHOR CONTRIBUTIONS
Writing - original draft: Yundo Jung. Writing - review & editing: Cho Long Kim. Conceptualization: MA Jeong, Cho Long Kim. Data curation: Yundo Jung, SSungyeon Jung, Seungcheol Yu, Mi Ae Jeong. Project administration: Cho Long Kim. Visualization: Sungyeon Jung, Seungcheol Yu. Investigation: Yundo Jung, Sungyeon Jung, Seungcheol Yu, Mi Ae Jeong. Supervision: Cho Long Kim.