INTRODUCTION
Sugammadex (Bridion, Merck Sharp and Dohme Corp., USA) is a reversal agent for steroidal neuromuscular blocking agents, such as rocuronium and vecuronium [1]. This drug directly reverses the neuromuscular-blocking effect of rocuronium by encapsulating the drug molecules. Any depth of neuromuscular blockade is reversed by an effective dose of sugammadex [2,3]. Conventional reversal agents, such as acetylcholinesterase inhibitors, do not have a direct reversal effect; these agents inhibit the breakdown of acetylcholine at the neuromuscular junction and thus indirectly enhance recovery from neuromuscular blockade [4]. Sugammadex is the only complete antagonist for rocuronium and vecuronium.
Sugammadex is not metabolized at all or only minimally metabolized, and is excreted rapidly by the kidney in healthy patients [5]. Highly significant correlations have been reported between plasma sugammadex and creatinine clearance, and between rocuronium and creatinine clearance in patients administered with rocuronium and sugammadex [6]. Rocuronium is eliminated by biliary and renal excretion, but clearance of rocuronium is limited to renal excretion when encapsulated by sugammadex [2].
The US Food and Drug Administration does not recommend the use of sugammadex in patients with severe renal impairment [7]. Although high-flux dialysis effectively removes sugammadex and the sugammadex-rocuronium complex, low-flux dialysis, which is a less common form of dialysis, does not significantly reduce the plasma concentration of sugammadex [5,8,9]. Therefore, reactivation of rocuronium due to dissociation of the rocuronium-sugammadex complex, the reappearance of neuromuscular blocking, and other as-yet-unknown adverse effects of residual sugammadex in plasma, such as long-term adverse immunological effects, are matters of concern. Several studies have been performed on the safety and efficacy of sugammadex in patients with renal impairment [10-15]. Despite the concerns described previously, clinicians often use sugammadex in patients with end-stage renal disease (ESRD) due to the benefits of sugammadex and based on several studies demonstrating its safety in patients with ESRD. This study was conducted to establish further evidence of the safety of sugammadex in patients with ESRD, by comparing 30-day mortality after surgery between the patients who received sugammadex and those who did not.
MATERIALS AND METHODS
The Institutional Review Board (IRB) approved this retrospective observational study (no. SCHUH 2020-08-007). The data analysis plan was filed with the IRB before any data were accessed. The requirement for informed consent was waived because of the retrospective study design. This article follows the Strengthening the Reporting of Observational Studies in Epidemiology guidelines [16].
We retrospectively collected the medical records of all patients with ESRD aged 18-90 years who were dependent on hemodialysis and underwent surgery under general anesthesia at a university hospital between January 2018 and December 2019. Patients who underwent emergency, cancer, cardiac, or transplantation surgery were excluded. The last surgery was included in the analysis when patients underwent multiple surgeries during the study period.
A total of 2,134 patients were eligible for this study, and their electronic medical records of the hospital were reviewed. Data on demographics (age, sex, and body mass index), preoperative laboratory tests (hemoglobin, platelet, international normalized ratio, activated partial thromboplastin time, blood urea nitrogen, creatinine, plasma sodium [Na], plasma potassium [K], plasma chloride [Cl], plasma albumin, plasma calcium [Ca], plasma phosphorus [P], hemoglobin A1c, aspartate aminotransferase [AST], and alanine aminotransferase [ALT]), comorbidities (hypertension, atrial fibrillation, current angina, previous myocardial infarction [MI], previous congestive heart failure, valvular heart disease, dilated cardiomyopathy, previous cerebrovascular attack, chronic obstructive pulmonary disease, and diabetes mellitus), left ventricular ejection fraction, anesthetic duration, the volume of intraoperative crystalloids, colloids administered, and blood loss, intraoperative transfusion, and packed red blood cells unit of transfusion were collected. The preoperative laboratory tests were conducted after dialysis. Patients who received sugammadex were included in the sugammadex group, and those who did not were included in the non-sugammadex group. The primary outcome was 30-day mortality according to the sugammadex administration, and the secondary outcomes were the 1-year mortality rate and causes of death according to the sugammadex administration. Mortality data were obtained from patient electronic medical records, and by submitting a data request to the Korean National Statistical Office (Microdata Integrated Service: https://mdis.kostat.go.kr). The mortality data of citizens of the Republic of Korea are comprehensively managed through resident registration numbers, as reflected in our statistics.
Our institution has a general anesthetic protocol. After placing the patient on the operating table, devices for electrocardiography, pulse oximetry, noninvasive blood pressure monitoring, neuromuscular transmission (NMT, General Electric Healthcare, Finland), and the bispectral index (BIS, Aspect Medical Systems, USA) were attached. Volatile anesthesia or total intravenous anesthesia was selected by the assigned anesthesiologist.
Volatile anesthesia was induced with 2% lidocaine (40 mg), 1% propofol (1-1.5 mg/kg), and rocuronium (0.6 mg/kg); if needed, remifentanil was administered using a target-controlled infusion system (Orchestra Primea, Fresenius Kabi AG, Germany) at a concentration of 0-6 ng/ml. Sevoflurane or desflurane was used for maintenance, and their doses were adjusted to maintain a BIS value of 40-60.
In cases of total intravenous anesthesia, 2% propofol and remifentanil were used to induce and maintain anesthesia using a target-controlled infusion system; the same regimen was used for lidocaine and rocuronium. The target-controlled infusion of propofol was adjusted (2-5 μg/ml) to maintain a BIS value of 40-60, and remifentanil was administered (0-6 ng/ml) during the operation. In both protocols, 4 mg of intravenous ephedrine or 50 μg of phenylephrine was used as necessary. Train-of-four monitoring using NMT continued throughout the whole period of anesthesia, but additional rocuronium was administered only when the patient moved or resisted mechanical ventilation, even if the train-of-four count exceeded 2. Fentanyl (0.3-0.5 μg/kg) was administered at the beginning of skin closure. At the end of the surgery, 0.2 mg/kg of pyridostigmine, and 5 μg/kg of glycopyrrolate or 1-2 mg/kg of sugammadex, was administered. The choice of reversal agent was at the discretion of the anesthesiologist. After confirmation of adequate reversal of neuromuscular blocking using NMT (train-of-four T4/T1 ratio of 0.9), the patient was extubated or the supraglottic airway was removed. After transfer to the post-anesthetic care unit, patients were observed for the presence of residual symptoms or the reappearance of neuromuscular blocking, and received an opioid or antiemetic as necessary. Patients transferred to the intensive care unit followed the post-operative patient management policy of the intensive care unit. Our institution uses only low-flux dialysis, and all patients received dialysis on postoperative day 0 or 1.
Patient demographics, comorbidities, laboratory test results, intraoperative recordings, and the 30-day and 1-year mortality rates were compared between the sugammadex and non-sugammadex groups using Mann-Whitney U test for continuous variables, and the chi-square (except for ‘dilated cardiomyopathy’) or Fisher’s exact test (only for ‘dilated cardiomyopathy’) for categorical data. The Shapiro-Wilk test was used to assess the normality of the data distribution. The propensity score matching method was used to correct for selection bias and adjust for confounding factors [17]. The factors included were a history of hypertension, atrial fibrillation, current angina, previous MI, previous congestive heart failure, valvular heart disease, dilated cardiomyopathy, previous cerebrovascular attack, chronic obstructive pulmonary disease, diabetes mellitus, and variables with significant differences (P < 0.05) between the groups. First, the propensity score matching method was used to balance the covariates between the two groups. All patients were matched in a 1:1 ratio in order of nearest neighbor. The caliper of nearest neighbor matching was 0.1. At this time, it was evaluated using standard mean difference (SMD), and 0.1 was considered for the success of matching. Second, covariates with SMD values greater than 0.1 were used as adjustment variables for the final model. The SMD was used to evaluate the covariates; those with a SMD ≥ 0.1 were considered significant.
After confirming that the groups were well-matched, logistic regression was performed to determine whether sugammadex was associated with an increase in 30-day and 1-year mortality. If the SMD was ≥ 0.1 after propensity score matching, it was included in the final model as a covariate. The results of the univariable and multivariable logistic regression analyses are presented as odds ratios (ORs) with 95% confidence intervals (CIs). All statistical analyses were performed using Rex software (version 3.0.3, RexSoft Inc., Korea) [18] based on R (version 4.0.0, R Foundation for Statistical Computing, Austria), and a 2-sided P value < 0.05 was considered significant.
RESULTS
Among 2,134 patients with ESRD who underwent surgery under general anesthesia, 2,039 were enrolled in the analysis (Fig. 1). Sugammadex was administered as a reversal agent for rocuronium in 806 (39.5%) patients, while 1,233 (60.5%) patients did not receive sugammadex. During propensity score matching, 12 patients were excluded because of missing data, and 2,027 were included in the matching. After propensity score matching, 797 patients were assigned to the sugammadex group and 797 patients to the non-sugammadex group (Fig. 1).
Table 1 shows the characteristics of the patients before and after propensity score matching, respectively. Age, sex, current angina, previous congestive heart failure, valvular heart disease, left ventricular ejection fraction, preoperative post-dialysis plasma K, Cl, albumin, and P, the amount of intraoperatively administered crystalloid, anesthetic duration and intraoperative transfusion were significantly different between the groups before matching. Because preoperative echocardiography was not performed in all patients, it was not considered in the matching process. No significant difference was observed between the groups after matching. As the number of patients who received blood transfusion was too small for propensity score matching, it was not considered in the matching process, but was included in the regression analysis. The SMD of factors with P < 0.05 (age, sex, plasma K, Cl, albumin and P, amount of intraoperatively administered crystalloid, and anesthetic duration) and of comorbidities (hypertension, atrial fibrillation, current angina, previous MI, previous congestive heart failure, valvular heart disease, dilated cardiomyopathy, previous cerebrovascular attack, chronic obstructive pulmonary disease, and diabetes mellitus) were calculated. The factors including a history of hypertension, atrial fibrillation, current angina, previous MI, previous congestive heart failure, valvular heart disease, dilated cardiomyopathy, previous cerebrovascular attack, chronic obstructive pulmonary disease, diabetes mellitus, and variables with significant differences (P < 0.05) between the groups[age, sex, plasma K, Cl, albumin, and P, amount of intraoperatively administered crystalloid, and anesthetic duration] were used in propensity score matching. After matching, all covariates except for the amount of intraoperatively administered crystalloid, anesthetic duration, and transfusion had a SMD < 0.1 in all 1,594 patients (Table 1, Supplementary Fig. 1).
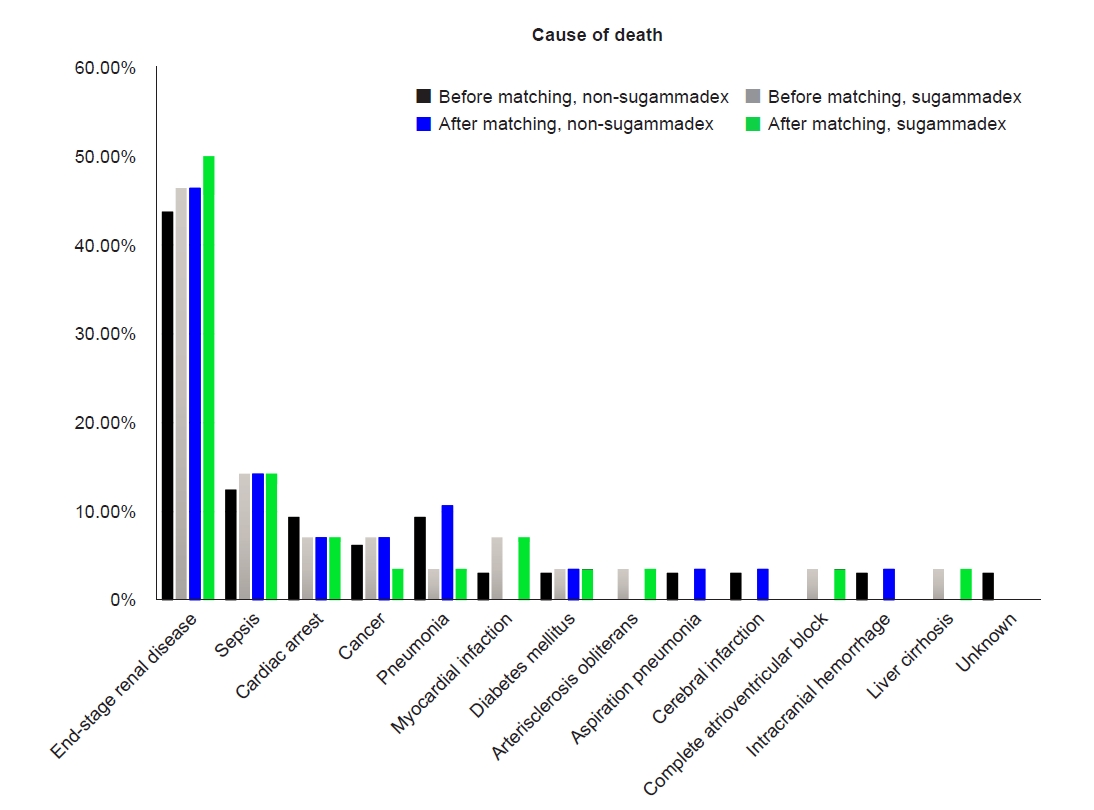
Table 2 shows the 30-day and 1-year mortality rates of both groups before and after propensity score matching. No significant difference in the 30-day or 1-year mortality rate was observed between the two groups before or after matching. After matching, 1,594 patients were analyzed; 28 (3.5%) of the 797 patients administered sugammadex, and 28 (3.5%) of the 797 patients without sugammadex, died within 30 days after surgery (P > 0.99); 38 (4.8%) of the 797 patients administered sugammadex, and 45 (5.7%) of the 797 patients without sugammadex, died within 1 year after surgery (P = 0.499) (Table 2). Additionally, no significant differences in the causes of 30-day mortality were observed between the two groups before matching (P = 0.982) or after matching (P = 0.860) (Fig. 2). The unadjusted OR of sugammadex for 30-day mortality was 1.01 (95% CI 0.59 to 1.72). The adjusted OR of sugammadex for 30-day mortality was 0.94 (95% CI 0.55 to 1.62), while for 1-year mortality it was 0.80 (95% CI 0.51 to 1.26) (Table 3).
DISCUSSION
Sugammadex was not significantly associated with 30-day or 1-year mortality after surgery under general anesthesia in more than 1,500 patients with ESRD. Although we did not detect any benefit of sugammadex, we could suggest that sugammadex does not increase mortality until one year after surgery.
It was reported the efficacy and safety of sugammadex for moderate neuromuscular blockade in patients with ESRD. The time to achieve a train-of-four T4/T1 ratio of 0.9 was no longer in patients with ESRD compared to normal controls, and 2 mg/kg sugammadex safely reversed the effects of rocuronium in patients with renal impairment [12]. However, efficacy and safety were only assessed 48 h after surgery and only for moderate neuromuscular blockade. In a later study, Staals et al. [6] reported that the plasma concentration of rocuronium did not differ between patients with severe renal impairment and controls before administering sugammadex. However, plasma clearance of rocuronium decreases significantly after administering sugammadex in patients with severe renal impairment [6]. Another study by Panhuizen et al. [11] demonstrated that 4 mg/kg sugammadex can safely and completely reverse neuromuscular blockade in patients with severe renal impairment, but recovery of the train-of-four T4/T1 ratio took longer than in controls. And the rocuronium-sugammadex complex remained at detectable levels in plasma on day 7 [11]. When encapsulated by sugammadex, clearance of rocuronium is limited to renal excretion [2]. Therefore, anesthesiologists may be concerned about potential long-term adverse effects of sugammadex and the rocuronium-sugammadex complex, so may avoid using sugammadex in patients with ESRD. There is a controversy about whether sugammadex can reduce postoperative pulmonary complications; there are studies proving that sugammadex could not reduce postoperative pulmonary outcomes [19,20]; on the other side, a study revealed that sugammadex significantly reduced pulmonary complications compared to neostigmine, including pneumonia and respiratory failure [21]. However, these studies did not perform subgroup analyzes of a patient with an American Society of Anesthesiologists physical status of 3-5. In patients with an American Society of Anesthesiologists physical status of 3-4, sugammadex significantly reduces the negative impact of older age on pulmonary outcome scores compared to neostigmine [22]. Furthermore, extubation after achieving a higher train-of-four ratio had a beneficial effect on postoperative pulmonary complications, and a higher train-of-four ratio was achieved more easily and reliably with sugammadex than neostigmine [23,24]. Sugammadex might have potential benefits in terms of safety for high-risk patients with an American Society of Anesthesiologists physical status of ≥ 3. Additionally, a meta-analysis showed that sugammadex significantly decreases the risk of bradycardia, and postoperative nausea and vomiting, as well as signs of postoperative residual paralysis [25]. Therefore, sugammadex has certain advantages, and there is no evidence that it worsens the postoperative mortality outcomes of patients with ESRD, either from our study or several previous studies [10-12,14,15,24].
Chronic kidney disease is an independent risk factor for postoperative mortality and complications [26]. In addition, most patients with ESRD have multiple comorbidities, including cardiovascular disease and diabetes mellitus [27]. Considering their severe comorbidities, the baseline characteristics of patients with ESRD could be important factors in mortality after surgery and anesthesia. Therefore, we used propensity score matching to adjust for these factors. In addition to comorbidities, preoperative laboratory test results, including sodium, potassium, chloride, albumin, and phosphorus plasma concentrations, were included as potential confounding variables [28-30].
Some limitations of this study should be discussed. First, there was no standard protocol for the use of sugammadex, because of the retrospective design of the study. The anesthesiologists decided at their discretion between pyridostigmine and sugammadex as the reversal agent for neuromuscular blockade. Selection bias would be caused by the anesthesiologist tending to use sugammadex in fragile patients who cannot recover easily from neuromuscular blockade. However, the purpose of this study was to determine the safety of sugammadex. The potential selection bias further emphasizes the benefits of sugammadex, where there was no difference in mortality between the sugammadex and non-sugammadex groups. Second, no significant differences in the causes of postoperative death within 30 days were observed between the groups, but there were many cases with unclear causes, classified as ‘unknown’ or ‘end-stage renal disease’. Cardiovascular events are well known as the major cause of death in patients with ESRD [26], but we could not confirm it due to the retrospective study design and incompleteness of the cause of death record. Third, the sample size was insufficient for good statistical power in this study. Because no previous studies have analyzed postoperative mortality in patients with ESRD according to the use of sugammadex, we could not calculate the required sample size. Based on our 30-day mortality data, the estimated required sample size was 5,801 for each group to achieve 80% power. Fourth, the type of surgery may also affect mortality, but we did not investigate the type. Finally, we could not report immediate postoperative pulmonary complications due to the nature of the study design. However, several studies have confirmed the short-term safety of sugammadex in patients with renal impairment [10-12,14], and one study reviewed 219 patients with chronic kidney disease stage 5 administered sugammadex which study suggested that sugammadex could be considered as an alternative reversal agent in patients with ESRD in aspects of complications and mortality within 30 postoperative days [15]. Outcomes of our study are only 30-day and 1-year mortality, but our study is a comparison study using the propensity score matching method, and the number of patients included in final analysis is 1,594.
In this retrospective analysis, sugammadex did not increase the 30-day and 1-year mortality rate in patients with ESRD after surgery under general anesthesia. Because it is a short-term study at a single center, there are limitations in applying it to all ESRD patients. Most patients with ESRD have multiple comorbidities and a high-risk status. Given the benefits of sugammadex in high-risk patients, we expect that sugammadex would be helpful in patients with ESRD.