Living-donor ABO-incompatible (ABOi) liver transplantation (LT) is now recognized as the only way to overcome blood type barriers and successfully expand donor pools [1]. However, in case of ABOi LT, hyperacute rejection could be occurred because of immune response by anti-A or anti-B antibodies [2]. Therapeutic plasma exchange (TPE) decreases the naturally occurring anti-A or anti-B isoagglutinin titer. However, TPE, on the morning of LT, is occasionally inevitable in TPE-resistant patients who struggle to lower anti-A or anti-B isoagglutinin titers [3]. The isoagglutinin titers should be dropped below 1:8 to avoid hyperacute rejection [4,5].
However, an excessive citrate load during TPE can cause hypocalcemia and hypomagnesemia and acid-base imbalances [6]. Therefore, metabolic alkalosis with compensatory hypercarbia and electrolyte disturbances occurred before LT [7,8]. If TPE was performed the day before surgery, patients may have time to correct acid-base imbalance and electrolyte disturbances by respiratory compensation or supplement of electrolytes. On the contrary, TPE was performed even on the day of surgery, this imbalance will be further exacerbated, which can cause severe arrhythmias and fatal outcomes.
We report on two ABOi LT cases including severe metabolic alkalosis and ventricular tachycardia who received TPE on the day of surgery. One case had a surprisingly high metabolic alkalosis of pH 7.73 immediately after tracheal intubation and the other had sudden ventricular tachycardia after surgical incision accompanied with severe hypokalemia of 1.8 mmol/L.
CASE REPORT
These case reports were approved by the Institutional Review Board (no. 2021-0691).
Case 1
A 58-year-old male with alcoholic cirrhosis (Model for End-Stage Liver Disease [MELD] score: 17) received ABOi LT with TPE on the operative morning. The initial isoagglutinin titer of the patient was 1:2,048, and even after TPE was performed eight times up to the day before surgery, the titer was 1:32. The 9th TPE was performed on the morning of surgery, with 29 units (replaced volume 4,759 ml) of fresh frozen plasma (FFP) replaced and an acid-citrate-dextrose solution used as an anticoagulant. LT was then performed, with the final titer of 1:8.
Room air arterial blood gas analysis (ABGA) (Table 1) was performed after entering the operating room. The arterial partial pressure of carbon dioxide (PaCO2) and bicarbonate (HCO3) were unexpectedly high and were reexamined after encouraging deep breathing. Although we tried to avoid an unintentional increase of minute ventilation during anesthesia induction and manual bagging, which may disrupt compensatory hypercarbia, we found that PaCO2 was decreased from 75 mmHg to 46 mmHg. Consequently, this caused uncompensated severe metabolic alkalosis (pH, 7.53 to 7.73) with sustained HCO3 retention (> 60 mmol/L). Severe hypokalemia (2.1 mEq/L) was also noted.
Case 2
A 39-year-old male with alcoholic cirrhosis (MELD score: 18) received ABOi LT with an 8th TPE the operative morning. The initial isoagglutinin titer of the patient was 1:4,096. The titer was 1:16, even though TPE was performed seven times until the day before surgery. Therefore, the 8th TPE was performed on the morning of surgery, with 20 units (replaced volume 3,287 ml) of FFP replaced and an acid-citrate-dextrose solution used as an anticoagulant. LT was then performed with the final titer of 1:8.
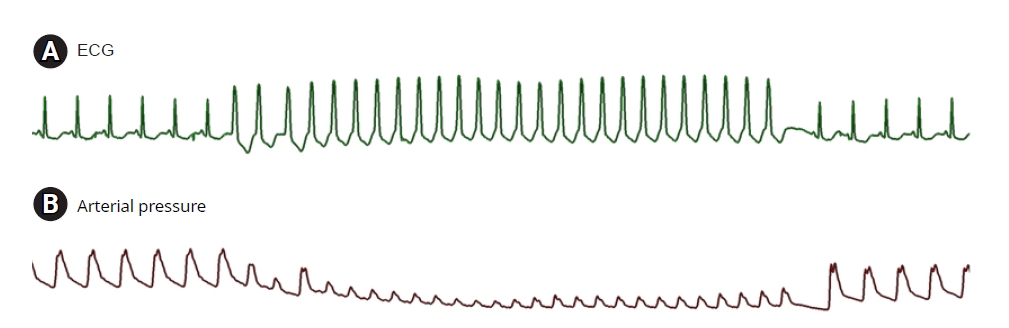
Metabolic alkalosis was revealed on room air ABGA (Table 2) after entering the operating room. Anesthesia was induced, with careful attention to avoid hyperventilation by bag and mask ventilation. After anesthesia induction, metabolic alkalosis and respiratory compensation were shown on ABGA with severe hypokalemia (1.8 mEq/L). Potassium chloride was supplemented, and hypokalemia was slightly resolved. However, ventricular tachycardia with severe blood pressure drop occurred for 10 s about 40 min after the incision, but the patient spontaneously recovered (Fig. 1).
DISCUSSION
According to the World Health Organization and the Spanish Transplant Organization, Organizaci├│n Nacional de Trasplantes Global Observatory on Donation and Transplantation, more than 30,000 LTs per year are performed worldwide as a potential curative treatment for patients with end-stage liver disease or hepatocellular carcinoma. However, a donor organ shortage in Korea has led to high waiting lists and increased mortality rates. Therefore, to overcome organ shortage, living-donor ABOi LTs have become increasingly popular [9,10].
Historically, ABOi LT has been challenged with various desensitization methods, such as TPE, direct graft infusion therapy, cyclophosphamide, splenectomy, and intraarterial or intravenous immunoglobulin therapies [2,8]. Currently, desensitization protocol of TPE with preemptive rituximab administration has been standardized and has allowed ABOi living donor liver transplantation (LDLT) to become more successful [1-3].
Pre-LT TPEs are typically performed many times until the day before LT to effectively decrease anti-A or anti-B isoagglutinin titers until dropped below 1:8 [4,5]. The titers were followed up daily before liver transplantation to ensure that the titer decreased below 1:8. Through the procedure, the incidence of hyperacute rejection in ABOi LT can be reduced. Usually, TPE was performed using a dual lumen central venous catheter in the internal jugular vein. The infusion rate was set at approximately 40 ml/min and was adjusted according to the patient's tolerance. Albumin, which role a significant part in blood osmotic pressure, was the preferred replacement fluid as long as coagulation lab test was within the normal range [11]. Regional citrate anticoagulation (RCA) was infused with a huge amount of FFP as replacement fluid. The FFP infused approximately 1.5 times the plasma volume [4]. The FFP can compensate for the loss of coagulation factors accompanied by plasma drainage. The RCA used in TPE, which was combined with ionized calcium, which was a necessary cofactor of the coagulation cascade [12]. Accumulation of citrate causes systemic hypocalcemia, which leads to tetany, QT prolongation and life-threatening arrhythmias may occur [13]. Therefore, during TPE, calcium gluconate was continuously infused to prevent hypocalcemia [14]. However, the massive citrate load from the RCA solution and FFPs might shift the acid-base status in liver cirrhosis patients from respiratory alkalosis to metabolic alkalosis [8]. Consequently, with pre-existing electrolyte disturbances, the risk of severe hypokalemia and hypomagnesemia are aggravated in ABOi LDLT recipients [8].
Therefore, anesthesiologists should be alert in patients with ABOi LT because inadvertent hyperventilation might take place during anesthesia induction with manual bagging. Such hyperventilation may lead to severe alkalosis because rapid respiratory alkalosis initiated by an unintentional fall in PaCO2 profoundly aggravates preexisting metabolic alkalosis by TPE [8].
In our first case, we were surprised to find that a pH of 7.7 and severe hypokalemia after tracheal intubation developed, even though we intended to avoid hyperventilation. This implies we should have paid more attention and been more careful during manual bagging. After finding this severe alkalosis, we decreased minute ventilation to compensate severe alkalosis and small amount of potassium chloride was supplemented.
Our second case developed ventricular tachycardia with severe hypokalemia (1.8 mmol/L) after surgical incision. Fortunately, the ventricular tachycardia running time was short and recovered spontaneously without treatment. We therefore could begin to manage the acid-base and electrolyte disturbances without further ventricular arrhythmias.
PotassiumŌĆÖs the arrhythmogenic potential on the heart has been extensively studied [15]. If severe, it is associated with life-threatening ventricular arrhythmias. Various literatures demonstrated a significant positive correlation between hypokalemia and the incidence of malignant ventricular arrhythmias. Therefore, in case of severe hypokalemia, potassium supplementation should be actively carried out within the recommended infusion rate.
The electrocardiographic (ECG) criteria for hypokalemia include the presence of U waves greater than 1 mm and U waves larger than the T wave with associated ST-segment depression [15]. Before developing ventricular tachycardia, our second case of hypokalemia also showed similar hypokalemic ECG changes.
In conclusion, our cases report strongly suggests that anesthesiologists should pay particular attention to PaCO2 changes and hypokalemia in ABOi LT, particularly at the start of anesthesia and mechanical ventilation in patients who just finished TPE the operative day morning. This may disturb the acid-base homeostasis and electrolyte balance, resulting in life-threatening ventricular tachycardia.