INTRODUCTION
Although first reported in 1981 [1,2], the term “ex-utero intrapartum treatment (EXIT)” was introduced in 1997 by a team that had successfully performed fetal surgery [3]. Also described as “operation on placental support” or “airway management on placental support”, EXIT allows surgical procedures or airway management in the fetus by maintaining uteroplacental circulation outside the uterus. Cesarean section is completed only after ensuring the neonate’s safety. It was first successfully applied to safely “unplug” fetuses treated using the PLUG (Plug the Lung Until it Grows) technique due to congenital diaphragmatic hernia (CDH) [3]. Mychaliska et al. [3] reported a series of six successful cases where EXIT was applied for the “unplug” phase, and two cases where EXIT was performed in fetuses diagnosed with neck masses. After identifying patients in need of EXIT, patient management begins with the creation of a multidisciplinary team that includes obstetricians, radiologists, obstetric anesthesiologists, pediatric surgeons, anesthesiologists, and neonatologists. Based on magnetic resonance imaging (MRI) findings [4], a multidisciplinary team must develop a plan before surgery to minimize confusion and prepare for multiple scenarios. The final decision regarding the direction of further treatment of the fetus or whether EXIT is necessary should be made by the multidisciplinary team. It is essential to plan and prepare the procedures. Although fetal management under EXIT can be performed for a considerable duration (150 min) [5], procedures should be performed quickly to avoid maternal infection. In the present review, we briefly overview the indications for EXIT and intraoperative maternal management, followed by a detailed review of intraoperative fetal management during EXIT.
INDICATIONS FOR EXIT
While EXIT can be used in patients with significantly compromised fetal airways, previous studies have suggested several indications, including airway displacement due to fetal neck mass [6], tracheal occlusion at delivery, tracheostomy for congenital high upper airway obstruction syndrome (CHAOS), surgical resection for thoracic abnormality, extracorporeal membrane oxygenation (ECMO) [7], and conjoined twins [8].
Airway displacement due to fetal neck mass (tracheoesophageal displacement index > 12 mm)
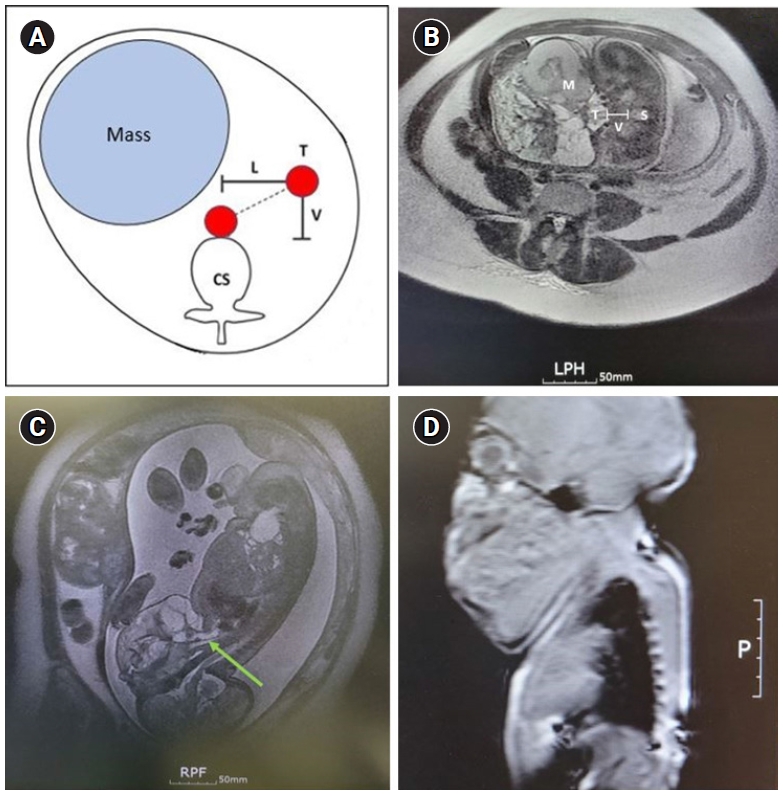
In fetuses with large neck masses, Lazar et al. [6] identified several characteristics predictive of airway difficulty, including polyhydramnios, diagnosis of teratoma, or a tracheoesophageal displacement index (TEDI) > 12 mm. Their data suggested that fetuses without these findings may be delivered safely without EXIT. TEDI is defined as the sum of the lateral (L) and ventral (V) displacements of the tracheoesophageal complex (T) from the ventral aspect of the cervical spine (S) on fetal MRI (Fig. 1). The fetus in Fig. 1 was planned for EXIT with a 17-mm TEDI, and endotracheal intubation was successful after three attempts using direct laryngoscopy for 9 min; tracheostomy was not required. In Fig. 1C, the fetal airway is filled with amniotic fluid, and the white shaded line (green arrow) connects to the lungs. Although the structure of the oral cavity cannot be predicted in detail, the airway is continuously maintained in the presence of fluid.
Tracheal occlusion state at delivery (PLUG state)
In the most severe cases of CDH, the liver occupies a large portion of the chest [9]. Right-sided hernia (10% of CDH) is challenging to diagnose owing to the difficulty of differentiating between CDH and other malformations such as congenital cystic adenomatoid malformation (CCAM). Metkus et al. [10] reported that fetuses with a lung-to-head ratio (LHR; lung area/head circumference) < 0.6 did not survive despite postnatal treatment, but the survival rate of fetuses with an LHR > 1.35 was 100%. LHR values < 1.0 are used to select fetuses for PLUG, which may help to grow their lungs and improve their outcomes. The tracheal occlusion procedure is commonly performed after a gestational age of 27-29 weeks to prevent the normal outflow of surfactant-rich fetal lung fluid. If this occurs over a period of 4-5 weeks, the lung expands, and its function appears to improve. Recently, as fetoscopy technology has improved, UNPLUG is performed 4-5 weeks after PLUG to avoid the risk of EXIT. If the fetus is in the proper position, the balloon is punctured under ultrasound guidance at approximately 34 weeks of gestation. The deflated balloon is subsequently expelled from the trachea by lung fluids. If needle puncturing is not possible, a grasper can be used to hold the balloon while it is punctured. The deflated balloon is then removed from the fetus’ airway using a grasper. The mother and fetus are subsequently monitored carefully until delivery. In this case, unlike with EXIT, vaginal delivery is possible at full term. If the fetus is in “PLUG” before delivery, “UNPLUG” is using EXIT.
Tracheostomy for congenital high upper airway obstruction syndrome
CHAOS, which manifests as a laryngeal web, cyst, or as tracheal or subglottic atresia, has a poorer prognosis than extrinsic lesions, such as a neck mass because the obstruction occurs earlier in gestation [11]. Without fetal intervention to relieve back pressure, the lungs do not develop properly, and ventilation and oxygenation cannot be achieved even after successful EXIT. Most fetuses with CHAOS require EXIT for tracheostomy [12].
Surgical resection for thoracic abnormality
CCAM, which accounts for more than 50% of congenital lung malformations, may also be an indication for EXIT. CCAM occurs during early embryonic development due to disorganization of peripheral bronchioles and adenomatous tissue proliferation. Renal dysplasia, congenital heart disease, foregut malformation, bronchogenic cysts, and skeletal malformations may also be present. Chromosomal abnormalities such as trisomy 13, 18, or 21 syndrome have also been reported [13]. Prognosis is mainly determined by the size of the mass. If the CCAM volume ratio (width × height × length × 0.523) is > 1.6, fetal hydrops is more likely to be present, and ECMO, as well as fetal intervention and ventilatory support, may be required [7]. Furthermore, a thoracoamniotic shunt for the largest cyst or premature delivery with EXIT may be required [14].
MATERNAL ANESTHESIA
It is now recognized that the key to successful EXIT is maintaining maximal relaxation of the uterus. Thus, neuraxial anesthesia, if used, should be combined with general anesthesia using volatile anesthetics. However, in rare cases where volatile anesthetics cannot be used (e.g., malignant hyperthermia), intravenous nitroglycerin should be continuously administered to relax the uterus [15]. Nitroglycerin can be maintained at a rate of 1-20 μg/kg/min after loading with 25-100 μg. Nitroglycerin is essential when anesthesia is maintained with only neuraxial anesthesia or total intravenous anesthesia [16]. Nitroglycerin is often used in general anesthesia with halogenated gas. In this case, dopamine (5-10 μg/kg/min) or phenylephrine is continuously administered to maintain blood pressure. It is safe to secure a central venous line for vasoactive drugs and blood transfusions while accurately monitoring arterial and venous pressures by securing arterial and central venous routes.
Most cesarean sections with EXIT are performed under general anesthesia with a volatile anesthetic agent. Relatively high doses of volatile agents should be used solely for uterine relaxation (2-3 MAC). However, due to the risk of a decrease in uterine blood flow, it is essential to maintain normal maternal blood pressure. Although both ephedrine and phenylephrine can be used, recent studies suggest the use of phenylephrine since ephedrine crosses the placenta more readily than phenylephrine [17]. The authors use sevoflurane, which can be administered at high concentrations, for inhalation gas and intermittently use ephedrine as needed, along with a continuous infusion of phenylephrine (10-50 μg/min). The maternal mean arterial pressure is maintained above 70 mmHg. After hysterotomy, the uterine cavity is filled continuously with warm (37°C) lactated Ringer solution using a fast-flow fluid warmer or pump to maintain adequate uterine volume and prevent compression of the umbilical cord. The fetal head, upper torso, and arms are exteriorized, while the rest of the body remains within the uterine cavity to maintain uterine volume and fetal temperature.
A previous study showed that postpartum wound complications were more common in patients who underwent EXIT than in those who underwent cesarean sections only (15% vs. 2%; P = 0.03) [18]. Estimated blood loss was higher in the patients who underwent EXIT (1,104 ml vs. 883 ml; P < 0.001), but there was no difference between groups with respect to hematocrit level change or postpartum hospital stay [18].
INTRAOPERATIVE FETAL MANAGEMENT
As the exact period when the fetus begins to feel pain remains uncertain, adequate analgesia should always be provided during EXIT procedures. Studies have also suggested that anesthesia is required to blunt the stress response in the fetus [19]. This is especially important when maternal anesthesia is accomplished using neuroaxial anesthesia without the use of volatile agents. In such cases, nitroglycerin and remifentanil are often infused to induce uterine relaxation and provide fetal analgesia and immobilization [20,21]. However, most EXIT procedures are performed under maternal general anesthesia while providing adequate uterine relaxation. Although adequate fetal anesthesia may be accomplished by placental passage of inhalant anesthetics, previous studies have also used intramuscular injections of anesthetics, opioids, muscle relaxants, and atropine (as premedication) to obtain optimal conditions [22]. George et al. [21] used intramuscular ketamine for fetal anesthesia. Rocuronium 1-3 mg/kg can be directly injected into the fetus if immobilization is required. The combination of medications (fentanyl 5-15 µg/kg, atropine 20 µg/kg, and vecuronium 0.1-0.4 mg/kg) can be drawn up in unit doses in a 1 ml syringe and can be administered to the fetus intramuscularly, intravascularly, or via the umbilical cord [12]. If EXIT is prolonged, this combination may be repeated every 45 min to ensure an adequate level of fetal anesthesia.
During EXIT, the fetus depends on uteroplacental support and is often in a critical condition. Full uterine relaxation is essential because changes in placental vascular tone significantly affect fetal cardiac output. Although fetal myocardial contractions are significantly weaker than in children, contractions can be increased by contractile agents or by increased preloading. Blood transfusions and fluid therapy may be necessary because of the small blood volume, low levels of coagulation factors, and less active baroreceptors that limit vasoconstriction in response to hypovolemia. It is also important to recognize the high risk of hypothermia from heat loss due to the relatively thin skin, which must be avoided. The additional pathophysiology of certain fetal malformations can also lead to serious damage. Therefore, continuous fetal monitoring should be performed during EXIT to evaluate the effects of anesthesia, surgical procedures, and possible circulatory insufficiency due to illness [23].
Fetal pulse oximetry monitoring is essential during EXIT. Although often difficult to measure, the pulse oximeter can be wrapped in foil on either fetal hand to minimize interference from bright lights in the operating room and to continuously monitor the oxygen saturation status and heart rate. Normal fetal oxygen saturation ranges from 40% to 70%, and prompt treatment is required when arterial saturation drops below 40%. Immediate action is also necessary when the fetal heart rate falls more than 20% below baseline or below 140 beats/min [23]. The anesthesiologist must first notify the surgeon of possible fetal distress and increase maternal inspired oxygen, optimize uteroplacental circulation by maintaining maternal blood pressure and heart rate, rule out aortocaval compression, and achieve uterine relaxation in the presence of uterine contractions. Surgeons should also reposition the fetus to resolve possible umbilical cord compression, increase the amniotic fluid volume, and rule out placental abruption. If fetal distress is not resolved, fetal resuscitation must be initiated.
Additional fetal monitoring during EXIT has also been shown to provide valuable information. Fetal echocardiography can characterize the fetal heart rate, chamber volume with heart contractions, capacity of the atrioventricular valves, and vascular stenosis. Fetal hemoglobin and blood gases can be routinely sampled from the umbilical artery and vein by the surgeon. The normal values of cord blood gas vary depending on several factors, including gestational age and delivery type. Although normal values for fetuses undergoing EXIT procedures have not been established, lower limits of pH 7.10 and −12 mmol/L base excess have been used [24]. Peripheral venous access can be difficult due to the small size of the patients, limited exposure, and impaired ability to properly position the baby at the surgical site. A properly inserted catheter may still fall out due to vernix caseosa on the skin and must be sutured in place. If veins are not accessible, drugs can be administered intramuscularly or through the cord blood path.
AIRWAY MANAGEMENT OF THE FETUS
According to a previous review [12], CHAOS is the only malformation that requires tracheostomy for laryngeal obstruction. No clear trend was observed for other malformations. In addition, there were no clear features of airway obstruction that could recommend one airway intervention over others. In cases of cervical teratoma, neither the magnitude nor the extent of anatomical distortion was predictive of the type of airway intervention used. Although endotracheal intubation under direct laryngoscopy is typically performed in cases without specific conditions (CHAOS), diverse airway equipment should be prepared after preoperative consultation with pediatricians and otolaryngologists. Doctors’ familiarity with airway equipment should also be considered, and it is important to discuss the scenario in advance and perform aseptic preparation by sterilizing all necessary equipment. Previous reports have shown that advanced airway interventions, including tracheostomy, rigid bronchoscopy, retrograde wire intubation, partial mass resection, and tracheostomy can be performed [19,25]. A possible scenario for fetal airway management is shown in Fig. 2.
Intubation under direct or video laryngoscopy
During the initial intubation attempt, it is helpful to check the overall structure and condition of the airway using a direct laryngoscope. Although starting with the smallest sized laryngoscopy blade and performing stepwise increases until the size of the tongue base is visible is recommended, using a size 2 or 3 Macintosh blade from the beginning may help quickly examine the structure of the airway in cases with a relatively large mass or mouth. If the mass is a vascular neoplasm in the oral cavity, more careful selection of the blade size is required, and it is better to determine it based on preoperative imaging analysis. When the size is appropriate, but the angle makes it difficult to visualize the vocal cords, a video laryngoscope of the same size can be used. Video laryngoscopes should also be aseptically prepared in advance so that various sizes can be used without delay. Video laryngoscopes can be used to help lift the fetus a little farther from the uterus, extend the angle of the fetus's neck, or push the mass to one side for better visibility of the vocal cords to enable image sharing with other medical staff. One study reported using a video laryngoscope in the first attempt at endotracheal intubation [26]. To confirm the proper position of the endotracheal tube, auscultation should be performed because single-lung ventilation cannot be ruled out using capnography. Ultrasound can also be used to determine the exact location of the tip of the endotracheal tube [27] or tracheostomy tube. Tube positioning must be confirmed before any deviation from umbilical circulation occurs, and the position of the tube should be confirmed using at least two methods.
Intubation with rigid bronchoscopy
Intubation can also be performed under rigid bronchoscopy in fetuses who undergo treatment for endoscopic tracheal occlusion due to severe diaphragmatic hernia [3,28]. After the bronchoscopic procedure is completed, only the bronchoscope is removed while holding the external endotracheal tube. By setting the telescope and tube size at 0° and 4 mm, respectively, the telescope can be inserted into a 3.0 endotracheal tube [29].
Use of laryngeal mask airways
Another possible strategy is the use of a supraglottic airway. Laryngeal mask airways (LMAs) have been suggested as an alternative method for establishing an airway during neonatal resuscitation [30]. Previous studies have also reported successful airway management in cases of failed endotracheal intubation under direct laryngoscopy during EXIT. Baker et al. reported achieving fiberoptic intubation through an LMA during EXIT in a fetus diagnosed with a dysgnathia complex [31]. Other studies have reported performing tracheostomy under ventilation with LMA insertion [32]. Although several studies have compared the efficiency of diverse LMAs in children [33], there are limited data in neonates [34].
Retrograde wire intubation
Since placental circulation is maintained during EXIT, it is possible to attempt retrograde intubation, which is less invasive than tracheostomy. However, there are several important limitations when performing retrograde intubation in neonates. For instance, due to the lack of a Murphy's eye in small endotracheal tubes, there is no way to increase the distance between the insertion site of the retrograde guide and the vocal cord [35]. In addition, because of the narrow inner diameter of the tube, only a suction catheter or guidewire sheath can be used as an anterograde guide. Although ultrathin fiberoptic bronchoscopes (outer diameter [OD] of 1.8 or 2.2 mm) can be placed inside a 3-mm tube, they cannot be used as anterograde guides because they lack working chambers and suction channels [36]. A 2.8-mm-OD bronchoscope that can be used to insert a 4-mm-inner diameter (ID) tube has a 1.2-mm channel, but there is often significant resistance when passing the retrograde guide. Fortunately, a 4 French central venous catheter guidewire can be used as a retrograde guide. It is important to confirm that the retrograde guide catheter can be properly inserted into the channel of the bronchoscope, acting as an anterograde guide.
Surgical airway management
Tracheostomy must be performed immediately if the intervention cannot be delayed. An otolaryngologist must be on standby in case of emergency situations. Although tracheostomy is more invasive than retrograde intubation, it does not independently affect infants’ language and cognitive development [37]. Performing a tracheostomy in newborns requires careful preparation and skill, as the trachea is narrow and difficult to position relative to that in adults. The anatomy of the fetus is often more difficult to navigate during EXIT, and it is crucial to find an access location using ultrasound in advance. Since there is a possibility that the airway is deviated to one side, it is important to identify the location and direction of the airway using MRI before EXIT and confirm the airway using ultrasound before the skin incision. Although both vertical and horizontal skin incisions can be used, a vertical tracheal incision over the third and fourth rings is recommended during tracheostomy [38]. Incisions should not be made over the cricoid cartilage or the first tracheal ring. Maintaining “stay sutures” for a week with 4/0 Prolene nonabsorbable suture provides stability and helps with “maturation.” After a week, the tube can be changed and the stay sutures removed. The smallest Shiley Tube has an ID of 3.0 and an OD of 4.5 mm, and Portex® and Bivona® (Smiths Medical, UK) products have also been developed with an ID of 2.5 mm [39]. If the depth from the skin to the tracheotomy site is increased due to large neck masses, the airway must be secured with an endotracheal tube. The tagging should be firm to prevent the tube from falling out after separation from the placenta or during transfer. If the airway is secured with a tracheostomy tube, a dedicated tape can be used, but it should be fixed firmly so that only one finger can pass under the tape. This prevents hypoxic damage or death due to accidental decannulation. Even after successful tracheostomy, continuous management after the procedure is very important. Warming and humidification should be continued, and tube suction should be performed every 30 min during the first day to prevent tube obstruction caused by secretion.
If direct access to the trachea is difficult due to a huge neck mass, partial resection of the mass may be necessary [8]. Decompression with aspiration may be useful for cystic lesions. If tracheostomy is successful with partial resection of the solid mass, an anesthesia machine capable of neonatal anesthesia and an extra operating room should be prepared and kept warm because additional surgery may be required. If the preoperative imaging evaluation suggests that this is highly probable, O-negative red blood cells should be prepared and an intravenous route should be secured to enable the delivery of medication and fluid therapy, as well as blood, to the newborn.
ECMO
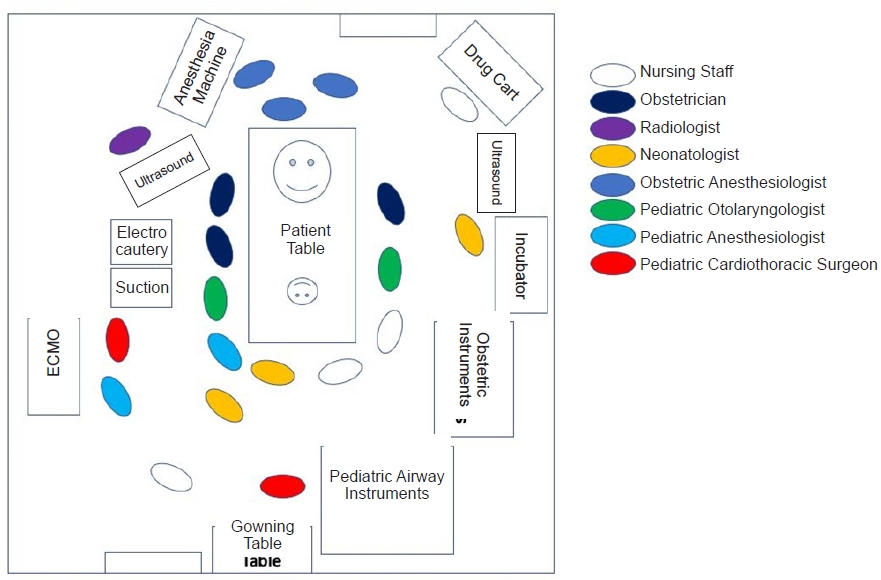
ECMO can be considered during EXIT in airways assessed to be extremely difficult. ECMO circulates blood through the carotid artery and internal jugular vein, and after the umbilical cord is clamped, an umbilical arterial and venous catheter is added to enable the ECMO circulation. The first study to provide a standard for neonatal ECMO treatment reported that 25 of 45 newborns with respiratory failure were saved using ECMO, and 20 of the 25 survivors subsequently exhibited normal lung function without brain damage [40]. For 14 fetuses diagnosed with severe CDH but who experienced PLUG failure, veno-arterial ECMO was applied using an 8 French arterial cannula and a 10 French venous cannula, and veno-venous ECMO was performed using a 12 French double-lumen cannula [41]. The authors reported a 1-year neonatal survival rate of 64%. However, the situation is significantly different in the presence of large neck masses. If the neck mass is large enough to make tracheostomy unfeasible or cause severe anatomical variation, it is highly possible that carotid artery and internal jugular vein access is also difficult, even after mass resection. In such cases, central ECMO through sternotomy may be necessary. As central ECMO requires multiple experts, including radiologists, obstetric anesthesiologists, obstetricians, pediatric surgeons, pediatric anesthesiologists, neonatologists, and pediatric thoracic surgeons, special attention is needed to prevent perioperative infection (Fig. 3).
CONCLUSION
The purpose of EXIT is to separate the fetus from the mother after resolving airway obstruction of the fetus while maintaining placental circulation. This can only be accomplished by a multidisciplinary team composed of experts who continuously discuss the optimal treatment method for the fetus. Anesthesiologists must be aware of the difficulties associated with airway management during EXIT and thoroughly prepare for multiple scenarios.