INTRODUCTION
Although there are several essential indications for central vein catheterization in small pediatric patients [1], catheterization is not easily achieved in these patients because of their small size and because the vessels can easily collapse. The subclavian vein, which runs underneath the clavicle and lies deeper than the internal jugular vein, is less collapsible and associated with a lower infection rate [2]. Subclavian vein catheterization can be performed safely and efficiently under real-time ultrasound guidance [3].
Central venous catheterization has been successfully performed in pediatric patients using a classical infraclavicular approach with ultrasound scanning at the supraclavicular level [4,5]. However, the optimal length of catheter insertion in pediatric patients undergoing subclavian venous catheterization has not been determined. Most methods suggested to date utilize an approach through the internal jugular vein or are less intuitive [6-9].
A simple landmark-based equation has been suggested for internal jugular vein catheterization [8]. This method allows a catheter tip to be positioned at the optimal target on chest radiographs [8,10]. This method does not require pre-procedural assessment of demographic or radiologic characteristics and the landmark-based distances can be easily measured during the procedure. However, this method has not yet been validated for subclavian catheterization. This study therefore retrospectively assessed the feasibility of the simple landmark-based equation in pediatric patients of corrected age < 1 year.
MATERIALS AND METHODS
Study design and population
The protocol of this retrospective study was approved by the Institutional Review Board of Chungnam National University Hospital (CNUH 2020-04-12), which waived the requirement for informed consent because of the retrospective nature of the study. The medical records and post-procedural notes recorded by the physician who performed the central catheterization via the right subclavian vein between 2016 and 2019 were reviewed. Patients were excluded if they were of corrected age > 1 year. Corrected age was calculated by subtracting the number of weeks born before 40 weeks of gestation from the chronological age [11]. Postmenstrual age was calculated by adding the gestational age and chronological age; thus, a 1-year-old infant born at full-term (gestational age 40 weeks) would have a postmenstrual age of 92 weeks.
Infraclavicular approach to the subclavian vein
All procedures were performed as described previously [5,8]. A linear ultrasound probe was placed at the supraclavicular level with the clavicle at the center of the view. The probe was then directed slightly inferolateral to the superomedial direction. Using an ultrasound-guided in-plane technique, the subclavian vein was punctured with an introducer needle via the infraclavicular route (Fig. 1B). A guidewire was inserted through the needle and the internal jugular vein was scanned to rule out cephalad insertion. The distances between the landmark points were measured during the procedure with a sterile ruler. These measurements included the distances from the needle insertion point (I) to the tip of the sternal head of the right clavicle (A) and from point A to the midpoint (B) of the perpendicular line drawn from the sternal head of the right clavicle to the line connecting the nipples (Fig. 1A). The initial insertion length was determined by adding the distances from I to A and from A to B and fixed after adjusting the length within a 1 cm range by considering the occurrence of an arrhythmia, resistance during aspiration, and the placement of an attachment clip.
Data acquisition
Landmark-based estimation has been used for catheterization in our center since 2016, and the measurements were included in post-procedural notes. Gestational age (weeks), chronological age (weeks), postmenstrual age (weeks), sex, birth weight, height, weight, length of the inserted catheter, and landmark related measurements (I to A [IA] and A to B [AB]) were recorded.
Anteroposterior chest radiographs were obtained after the procedure and reviewed by one author. The vertical distance from the carina to the CVC tip was measured using the Picture Archiving and Communicating System (PACS) (Maroview, Marosis, Korea). The optimal insertion length, defined as the distance at which the catheter tip was positioned at the level of the carina, was calculated as the actual inserted length ± the vertical distance between the catheter tip and the carina (Fig. 2). Correction for vertical distance was based on the consideration that the catheter usually runs vertically from the superior vena cava to the right atrium.
Derivation of the estimation method
Landmark-based estimations (IA + AB) were compared with determined optimal insertion lengths (actual inserted length ± vertical distance). These estimates were subsequently adjusted by determining the optimal intercept that minimizes the mean difference between the determined and estimated optimal insertion lengths.
To determine whether a more precise estimate can be derived from the data of the present study, a regression model was derived by a multiple linear regression analysis that included patient characteristics such as sex, height, weight, birth weight, chronological age, gestational age, postmenstrual age, IA, and AB. Variables with P values < 0.1 on univariate analysis were included in a multivariate analysis. When multicollinearity was detected (based on a variance inflation factor > 10), the more clinically meaningful or practical variable was selected. Finally, a model with the lowest Mallow’s Cp was chosen using a best subset selection approach.
Statistical analysis
The sample size was based on the available data from January 2016 to December 2019. No statistical power calculation was performed before the study. Statistical analysis was performed using R software version 4.0.3 (R Project for Statistical Computing, Austria). Continuous variables are presented as mean ± standard deviation (SD), with 95% confidence interval (CI), or medians and interquartile ranges (IQR) after testing for normal distribution using the Shapiro-Wilk test. The determined and estimated optimal insertion lengths were compared using the Bland-Altman method, which describes agreement between two quantitative measurements [12]. The mean difference (estimated - determined optimal length of insertion) and the 95% limits of agreement (± 1.96 SD of the difference) were calculated. A clinically acceptable limit was not defined a priori. The estimates from the landmark-based equation and the linear regression model were compared using paired t-tests. Two-tailed P values < 0.05 were considered statistically significant.
RESULTS
Of the 51 right subclavian catheterizations performed in 42 pediatric patients, one catheterization was excluded because of patient age. Thus, this analysis included 50 catheterizations in 41 patients (Fig. 3); their demographic and clinical characteristics are summarized in Table 1.
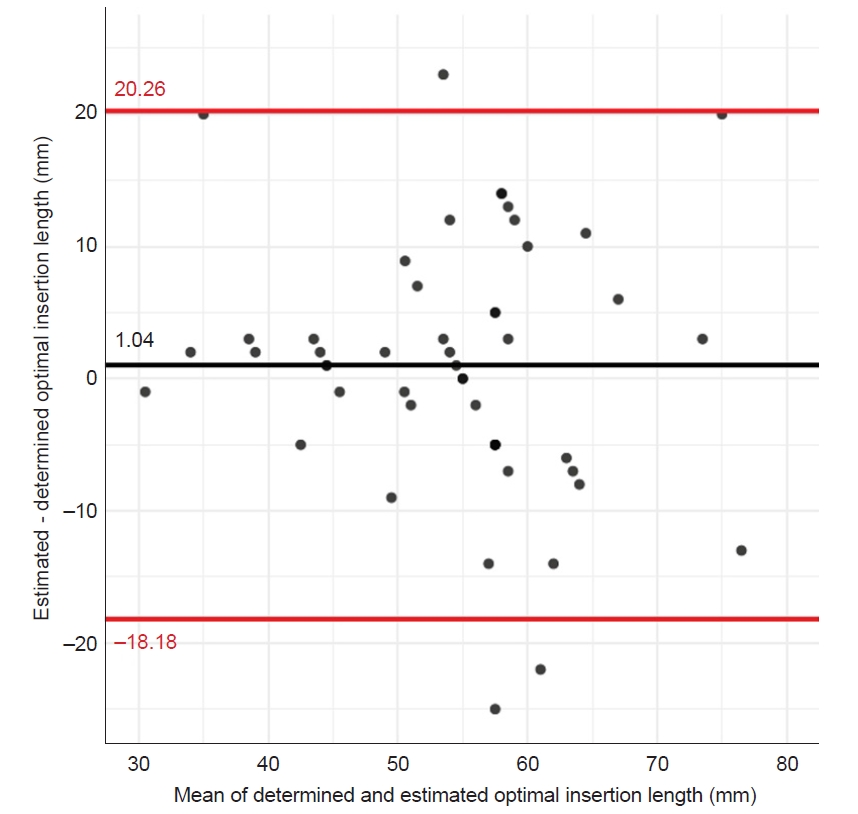
The difference between the optimal insertion length and the initial landmark-based estimation (IA + AB) was 6.04 ± 9.81 mm. For practical reasons, 5 mm was subtracted from each estimate (R2 = 0.361). The comparison between the determined optimal insertion length and the adjusted result (IA + AB - 5) is shown in Fig. 4. The mean difference was 1.04 mm, with the 95% limits of agreement being -18.18 mm and 20.26 mm.
Results of univariate and multivariate analyses are presented in Table 2. In the final model, postmenstrual age (weeks), weight (kg), IA (mm), and AB (mm) were selected, with predicted length calculated as 26.681 - 4.014 × weight + 0.576 × IA + 0.537 × AB - 0.482 × postmenstrual age (P < 0.001, adjusted R2 = 0. 396). A comparison between the determined optimal insertion length and the estimates using the final model is shown in Fig. 5. The mean difference was 0 mm and the 95% limits of agreement were -16.66 mm and 16.66 mm.
The difference between the estimates using the landmark-based equation and the linear regression model was not significant (mean difference -1.04 mm, 95% CI -2.43 to 0.35 mm).
DISCUSSION
This study compared the ability of two models, a landmark-based model and a linear regression model, to predict optimal insertion length during right subclavian vein catheterization in pediatric patients of corrected age < 1 year. Based on Bland-Altman analysis, the linear regression model was slightly more accurate than the simple landmark-based method. For practical reasons, however, we suggest that a simple landmark-based method be used rather than an estimation based on complicated calculations. The results of the present study indicate that, with a slight adjustment, clinicians can estimate the optimal insertion length by simple measurement and arithmetic. This simplicity may enhance the applicability of the method.
Several other methods have been suggested to determine the optimal insertion length of central catheters [7,13-15]. Most of these methods, however, are based on demographic data, may not be intuitive, and/or require complicated intraoperative calculations. Additionally, these methods may not include considerations of inevitable variations due to actual puncture sites. Based on the results of our multivariate analysis, the actual puncture site (IA) was the most important variable for estimating optimal insertion length. In this context, we considered the method suggested by Na et al. [8] (a method that includes the insertion point as an aspect of estimation) practical and also applicable to subclavian vein catheterization. To prevent inconsistencies between predetermined and actual puncture sites, measurements based on landmark points were performed using a sterile ruler immediately after the guidewire was introduced into the vascular lumen.
The infraclavicular approach to the subclavian vein has several advantages over internal jugular vein catheterization in infants [4]. During cannulation, the internal jugular vein tends to collapse easily in response to pressure from the probe or needle. Moreover, multiple attempts to perform internal jugular vein cannulation can result in hematoma around the blood vessels. In contrast, the subclavian vein is less prone to collapse during cannulation because it is suspended within the soft tissue underlying the clavicle [16]. Also, the infraclavicular approach allows direct visualization of needle advancement, reducing the risk of complications and improving the rate of successful placement. An ordinary linear probe, instead of a hockey-stick shaped probe, was shown to be successful in the infraclavicular approach for infants [5]. However, a skilled in-plane technique is required to prevent serious complications in these small infants.
The optimal position of the central catheter tip remains unclear [17]. Vessel injury and thrombosis may be avoided and proper functioning of the catheter maintained by positioning the catheter tip in the right atrium [18]. However, various problems are associated with deep catheter insertion, including arrhythmia, endocardial injury, and even cardiac perforation and tamponade [19-21]. Critically ill pediatric patients who require central catheterization are especially fragile, making prediction of the optimal insertion length imperative, even for guidewire insertion [22,23]. The wire should not be too deep, which may cause endocardial injury or arrhythmia, or too shallow, which may result in sub-optimal insertion of the catheter into the superior vena cava. Special caution is needed when inserting a straight-tip rather than a j-tip wire [24].
Whether deep or not, the actual intended length of catheter insertion should be based on accurate prediction. The suggested target point of the catheter tip in this study, the carina, can be considered a safe target. The average distance between the carina and the junction of the superior vena cava and right atrium in infants and children undergoing heart surgery has been reported to be 1.5 cm (95% CI 1.3-1.8 cm) [10], with this range (1.3 to 1.8 cm) constituting the clinically acceptable positive limit of error (i.e., estimate - determined value > 0). Based on this consideration accurate than the landmark-based method. Nevertheless, however, we concluded that the landmark-based method is also feasible in clinical practice, as the mean difference between the two estimates was -1.038 (95% CI -2.4 to 0.4 mm), making them clinically identical. Also, the estimation based on the regression model requires complicated calculations, which are difficult to be performed intraoperatively. In contrast, the landmark-based method can simply estimate optimal insertion length using intraoperatively measured variables.
This study had several limitations. First, the data used in this study were not purposefully collected. Therefore, information regarding detailed complications and accompanying congenital anomalies was not recorded. Second, several patients required repeated catheterizations. Despite the time gap between procedures, autocorrelation cannot be ruled out. Third, this was a single-center study, with all procedures performed by a single clinician. Our suggested method requires external validation. Fourth, based on the limits of agreement between the estimates and the determined optimal lengths of insertion, the estimation should be regarded as a guide rather than an absolute target.
In conclusion, this study suggests that a simple landmark-based method (IA + AB - 5) can estimate the optimal insertion length of the right subclavian vein catheterization in pediatric patients of corrected age < 1 year.