INTRODUCTION
Arterial pressure monitoring is essential for the management of hemodynamically unstable patients. The placement of an arterial catheter is sometimes technically challenging because some arteries have small calibers, anatomic variations, or arterial calcifications, or vasospasms. Multiple cannulation attempts are associated with a higher failure rate and complications such as hematoma, hemorrhage, vasospasm, occlusion, and infection. Ultrasonography is a useful tool for peripheral arterial catheterization [1]. Ultrasound guidance has been shown to facilitate arterial catheterization with fewer attempts. Ultrasound guidance for arterial catheterization improves the first and second attempt success rates and decreases the rate of complications compared to palpation or Doppler auditory assistance [2]. In addition, ultrasonography is a good modality for evaluating the extent of the artery in vasospasm as well as relaxation of the spasm after treatment [3]. This review deals with the anatomy of arteries, several ultrasound-guided arterial cannulation techniques, as well as tips to improve success rates and decrease complications associated with arterial catheterization.
ANATOMY
Upper extremity
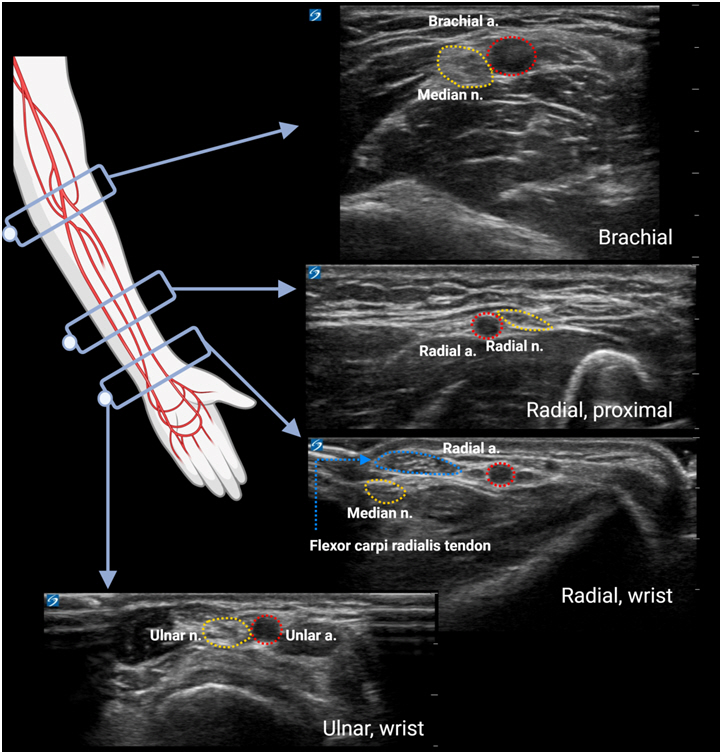
The radial, ulnar, and brachial arteries can be used for arterial catheterization of the upper extremity (Fig. 1). When an arterial catheter is placed at the upper extremity that is supplied with blood by the aberrant subclavian artery, it should be considered that arterial pressure may be underestimated by compression in its retroesophageal course. If the patient has an interrupted aortic arch, coarctation of the aorta, or Blalock-Tausig shunt, it should be noted that the pressure measured from the upper extremity may not accurately represent the systemic arterial pressures at other sites.
1. Radial artery
The radial artery is the most commonly preferred site for arterial catheterization [4,5] because of adequate collateral blood supply, low complication rates, and easy accessibility. The average diameter of the radial artery in adults and children is 2.2-2.3 ± 0.4 mm [6,7] and 1.2-1.3 ± 0.2 mm [8,9], respectively. The average depth of the radial artery from the skin in adults and children is 2.5 ± 0.3 mm [10] and 2.3 ± 0.7 mm [8], respectively. The radial artery originates from the brachial artery and reaches the lateral side of the wrist [11]. After the radial artery divides into the superficial and deep branches at the styloid process level of the radial head, the radial and ulnar arteries are connected with the superficial palmar and deep palmar arches. As some cases reported absent or dual radial arteries [11], prescanning with ultrasound before radial arterial catheterization or real-time ultrasound-guided procedure is recommended [12]. Since the modified Allen’s test has been debated as having low sensitivity to detect patency of collateral circulation [13], a recent guideline by the European Society of Anaesthesiology recommends performing the modified Allen’s test using ultrasound and color Doppler before radial artery catheterization [12].
2. Ulnar artery
The ulnar artery is relatively smaller than the radial artery in the palpable region of the wrist, although it is larger than the radial artery at the division site just below the elbow. The average diameter of the ulnar artery in adults is 2.3-2.5 ± 0.5 mm [6,7,14], which is smaller than the radial artery at the wrist level. The ulnar artery is a branch of the brachial artery and runs along the medial side of the wrist. The artery is located lateral to the ulnar nerve and flexor carpi ulnaris tendon in the palpable region of the wrist. Because the ulnar artery is also connected to the radial artery through the palmar arch, the modified Allen’s test with ultrasound would be helpful in preventing vascular complications [12].
3. Brachial artery
Brachial arteries are usually not recommended for cannulation because of the absence of collateral flow. However, the brachial artery could be considered for cannulation in neonates and small children [15], The average diameter of the brachial artery above the antecubital fossa is 3.9 ± 0.5 mm in adults [16] and 3.4 ± 0.2 mm in children [17]. The palpable site of the brachial artery is on the medial side of the biceps tendon on the anterior part of the elbow. Usually, the median nerve runs together medially with the brachial artery on the elbow. It is vulnerable to damage when the blind technique is used for brachial artery cannulation.
Lower extremity
The dorsalis pedis, posterior tibial, and femoral arteries can be used for arterial catheterization of the lower extremities (Fig. 2).
1. Dorsalis pedis artery
The dorsalis pedis artery is representative of the arterial cannulation site on the anterior side of the foot and originates from the anterior tibial artery. The diameter of the dorsalis pedis artery in adults and children is 3.0-3.6 ± 1.2 mm [18] and 1.0-1.3 ± 0.2 mm [8,19], respectively. Its depth from the skin surface in children is 2.5 ± 0.9 mm [8]. The landmark for its palpation is the most prominent part of the navicular bone and extensor hallucis longus tendon. The deep peroneal nerve is usually located lateral to the dorsalis pedis artery, with anatomical variations.
2. Posterior tibial artery
The posterior tibial artery is a reasonable alternative to the radial artery for ultrasound-guided arterial cannulation in small children [8]. The diameter of the posterior tibial artery is 3.1 ± 0.4 mm [20] in adults and 1.4 ± 0.3 mm in children [8]. Its depth from the skin surface is 3.4 ± 1.2 mm in children [8], which is located deeper than other peripheral arteries. It originates from the popliteal artery and runs along the medial border of the fibula, along with the posterior tibial vein and tibial nerve. The most palpable site of the posterior tibial artery, called Pimenta’s point, is found between the medial malleolus and the Achilles tendon. This artery is connected to the anterior tibial and peroneal arteries. Its depth from the skin surface decreases as the position of the ankle changes (e.g., dorsiflexion or eversion) [8]. Dorsiflexion of the ankle is helpful in posterior tibial arterial cannulation.
3. Femoral artery
The femoral artery is the largest accessible artery for arterial catheterization and continues from the external iliac and common iliac arteries. Because femoral arterial pressure represents the central arterial pressure, femoral arterial catheterization is useful in cardiopulmonary bypass [21,22] or liver transplantation [23], when peripheral arterial pressure monitoring does not reflect central blood pressure. The average diameter of the common-, superficial-, and deep-femoral artery in adults is 6.6 ± 1.2 mm, 5.2 ± 1.2 mm, 4.9 ± 0.9 mm [24], respectively. The average diameter of the pediatric femoral artery is 2.8 ± 0.8 mm in those aged 0-1 months, and increases to 5.6 ± 1.1 mm in those aged 5-7 years at 1 cm distal to the inguinal ligament [25]. The most palpable site of the femoral artery is under the inguinal ligament, between the anterior superior iliac crest and the pubic bone. Since the femoral artery is located between the femoral nerve (laterally) and femoral vein (medially) [26], femoral arterial catheterization with a blind technique is risky and increases complication rates. Therefore, ultrasound-guided femoral arterial catheterization is recommended in adults and children for safe and easier catheterization [12]. Moreover, as the overlap of the femoral vein increases by approximately 55% when it runs distal to the inguinal ligament, ultrasound-guided catheterization has been increasingly used [25]. External rotation of the hip joint can decrease femoral artery and vein overlapping. Femoral arterial catheterization should be performed carefully because serious complications, such as retroperitoneal hemorrhage or intra-abdominal organ injury, can occur.
ULTRASOUND-GUIDED TECHNIQUES
Ultrasound-guided arterial cannulation improves success rates and reduces procedural time and procedure-related complications compared with the direct pulse palpation method [1,12,27-29]. Ultrasound guidance is particularly useful when it is difficult to feel the arterial pulse, the arteries have small diameters (pediatric patients) or deep locations (obese patient), as well as in dehydration, hypotension, low cardiac output, non-pulsatile blood flow, vascular disease, and previously unsuccessful arterial cannulation [12,27].
A successful first cannulation attempt is important [9,30]. Failed cannulation attempts can cause arterial vasospasm, intra-arterial or extra-arterial hematoma, and further decrease the overall success rate. Multiple cannulation attempts can cause serious complications such as nerve injury, pseudoaneurysm, total arterial occlusion, and permanent distal ischemia [12]. Therefore, pre-procedural sonographic evaluation should be performed to identify the artery with the largest diameter, optimal depth, and straight course to increase the first-attempt success rate.
A high-frequency linear transducer or a hockey stick-shaped transducer is used to visualize the artery. A small hockey stick-shaped transducer helps to adjust the alignment of the needle and artery in pediatric patients. Duplex ultrasonography and color Doppler can be used to identify arterial pulses and to perform a modified Allen’s test before radial artery cannulation [31,32].
After choosing the target artery, it is important to adjust the height of the table and the location of the ultrasound machine so that the operator can perform arterial cannulation in a comfortable position. The operator then optimizes the patient’s wrist or ankle posture and fixes the joint so that cannulation can be performed without movement in the target artery. The depth and diameter of the target artery should be considered when selecting the size of the arterial catheter. Hand hygiene should be performed before gloving. An alcohol-based chlorhexidine antiseptic is recommended for skin preparation. When a sterile sheath is used, the transducer should be placed inside the sterile sheath carefully to prevent air from entering between the transducer and sheath.
There are two basic ultrasound-guided approaches: the short-axis view (SAX) out-of-plane approach and the long-axis view (LAX) in-plane approach. Moreover, some studies have proposed an oblique approach [20,33]. For radial artery cannulation, the currently available literature suggests similar success rates with either the SAX out-of-plane approach or the LAX in-plane approach in adults [34-36] and pediatric patients [37].
Short axis view out-of-plane approach
In the SAX out-of-plane approach, the transducer is placed perpendicular to the course of the target artery. The course and condition of the target artery can be checked by moving the transducer proximally and distally. In a good SAX, the target artery should appear as a pulsatile anechoic circle at the center of the screen. The needle is inserted approximately 30° to 45° to the skin and perpendicular to the center of the transducer. The middle mark on the ultrasound probe corresponding to the middle mark in the ultrasound image is helpful for inserting the catheter needle into the center of the target artery. The needle appeared as a hyperechoic dot and advanced until the anterior wall of the target artery collapses. If the needle tip is not visualized well, slight tiling or movement of the transducer will be helpful. When the needle enters the lumen of the artery, the collapsed anterior wall re-expands and flashback of the blood occurs (Fig. 3A, B).
The advantages of the SAX out-of-plane approach include: 1) easy scanning of the target artery, 2) easy maintenance of the transducer during the procedure, and 3) easy directing of the needle toward the target artery. The disadvantages of the SAX out-of-plane approach include 1) non-visualization of the entire course of the artery, 2) possibly not being able to visualize the needle tip on the ultrasound screen, and therefore, 3) cause possible puncture of the arterial posterior wall of the arterial posterior wall or misplacement of the needle tip behind the scene.
Modified short axis view out-of-plane approach
1. The ultrasound-guided dynamic needle tip positioning technique
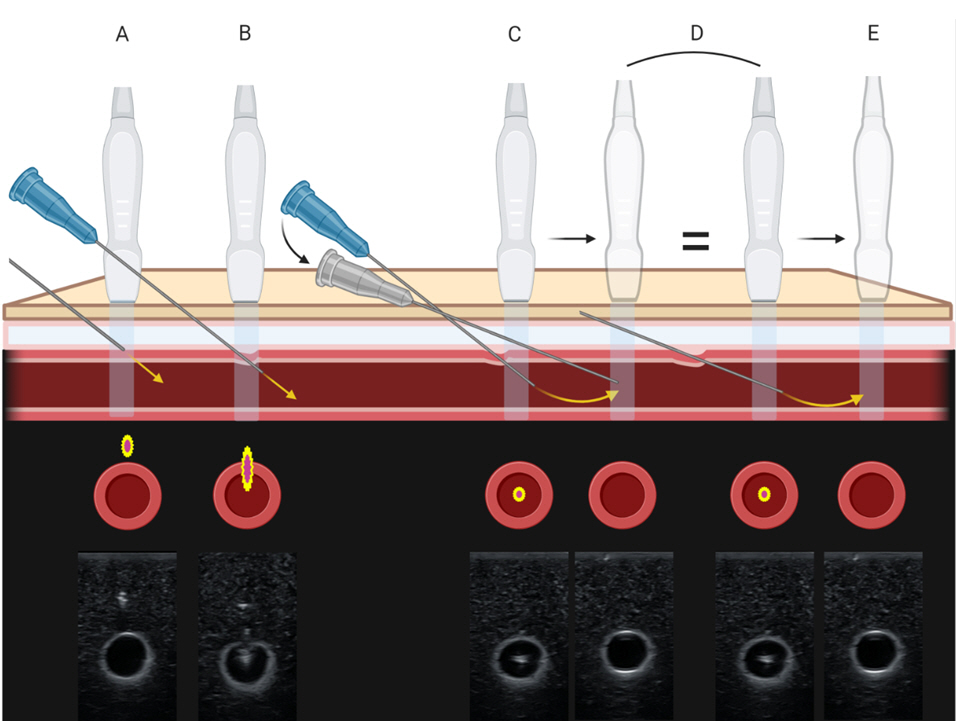
The ultrasound-guided dynamic needle tip positioning technique has been proposed to overcome the shortcomings of the SAX out-of-plane approach while maintaining its advantages. The needle tip of the shaft is displayed as a hyperechoic dot on the screen, and this dot can be more easily identified by adjusting the angle of needle insertion into the skin. The needle tip can be identified in the SAX by moving and tracing the probe. After puncturing the anterior wall of the artery and confirming the hyperechoic dot in the vessel lumen, the probe is moved proximally until the needle tip disappears and then the needle is slightly advanced until the hyperechoic dot reappears. This procedure is repeated until the needle with the catheter is fully inserted into the artery. In this procedure, the angle of needle advancement should be lower than the insertion angle concerning the course of the artery so as not to puncture the posterior wall of the artery (Fig. 3C-E). This technique increased the first and overall success rates compared to palpation in both adults and children [38-40].
2. Line on the probe for the midpoint
This method is advantageous for aligning the center of the transducer with the needle insertion point and the center of the artery. A developing line tied to the midpoint of the ultrasound probe and perpendicular to the long axis may improve the success rate of cannula insertion into the radial artery on the first attempt [35]. Acoustic shadowing via the use of double developing lines significantly improved the success rate of radial artery puncture in young children compared with that achieved using traditional ultrasound guidance [41].
Long axis view in-plane approach
In the LAX in-plane approach, the transducer is placed parallel to the course of the target artery. First, the target artery is scanned in SAX to capture the artery at the center of the screen. Then, the transducer is rotated by 90° while keeping the artery at the center of the screen. In a good LAX, the target artery should appear as a pulsatile tubular anechoic structure across the screen. The needle is inserted approximately 30° to 45° to the skin and perpendicular to the center of the longitudinally applied transducer. The needle appears as a hyperechoic double line above the artery and is advanced until the anterior wall of the target artery is punctured. If the needle tip is not visualized well, slight tilting of the needle to the left or right would be helpful. When the needle tip enters the lumen of the artery, the collapsed anterior wall re-expands and flashbacks of the blood will occur (Fig. 4).
The major advantage of the LAX in-plane approach is that the course of the artery and needle tip can be observed throughout the procedure. Therefore, puncture of the posterior arterial wall or misplacement of the needle tip is less likely to occur. The disadvantages of the LAX in-plane approach include 1) difficulty in identifying whether the needle is on the right or left side of the artery and 2) difficulty in maintaining transducer position as well as alignment of the needle shaft, tip, and artery during the procedure. Although we assume that the image plane of the ultrasound machine is paper-thin, the ultrasound beam has a measurable thickness. This is called a slice-thickness artifact. Therefore, the needle and target artery can appear on the screen in the LAX even though they are not exactly on the same plane [42]. Sometimes, the needle can be seen in the lumen of the target artery without a puncture. Therefore, it is important to confirm that the anterior wall of the target artery collapses during needle advancement. The LAX in-plane approach requires a longer imaging time, but the total time to cannulation is not different from that of the SAX approach. The posterior wall puncture rate is lower in the LAX in-plane approach than in the conventional SAX out-of-plane approach in children younger than 5 years of age [37].
Oblique approach
In the oblique approach, the transducer is placed parallel to the course of the target artery to obtain the image in the LAX. Then, the transducer is rotated from 10° to 15° while keeping the artery at the center of the screen [20,33]. In a good oblique view, the target artery should appear as a pulsatile elliptical anechoic structure across the screen. The needle is inserted through the skin and the target artery similar to the LAX approach (Fig. 5). In adults, the oblique approach showed a higher first-attempt success rate and, shorter procedure time, and less vasospasm and hematoma than the SAX out-of-plane or LAX in-plane approach [20,33,43]. The advantages of the oblique approach are as follows: 1) ease of scanning the target artery and 2) visualization of the needle with fewer section-thickness artifacts.
Other methods to improve success rates
1. Nitroglycerin
Nitroglycerin dilates the radial artery and decreases the incidence of vasospasm [9,44-47]. In adult patients, nitroglycerin has been used for radial artery dilation by intra-arterial [48,49], topical [50,51], and subcutaneous administration [44,46]. Application of topical nitroglycerin cream 30 min before radial artery cannulation has the advantage of being non-invasive and having significant vasodilatory effects on the radial artery in healthy adult patients [50,51]. Subcutaneous administration (500 μg) is effective for localized vasodilation without causing systemic side effects [44,46], and decreases the incidence of early radial artery occlusion after transradial coronary catheterization [47]. Radial artery cannulation can be difficult in infants and young children because of their small vessel sizes, with multiple attempts leading to vasospasm, hematoma, or a further decrease in the diameter of the artery. Subcutaneous nitroglycerin (5 μg/kg in 0.5 ml) injection before radial artery cannulation improves the first-attempt success rate and reduces overall complication rates in pediatric patients younger than 2 years [9].
2. Bevel orientation
The orientation of the needle bevel can affect the ultrasound image of the needle tip when using the LAX in-plane approach. When the bevel-down approach is used, the needle tip is at the end of one long line on the image, while in the bevel-up approach, the needle tip is at the end of another short line called the “bevel line”, which is observed in front and below the main long needle line. Neglecting to visualize the “bevel line” can result in inadvertent perforation of the posterior wall [52].
The bevel-down during ultrasound-guided SAX out-of-plane approach for radial artery catheterization exhibited a higher success rate with fewer complications compared to the bevel-up approach. Compared to the bevel-up approach, the bevel-down approach decreases posterior arterial wall injury in adults [10].
3. Technique after the flashback of the blood
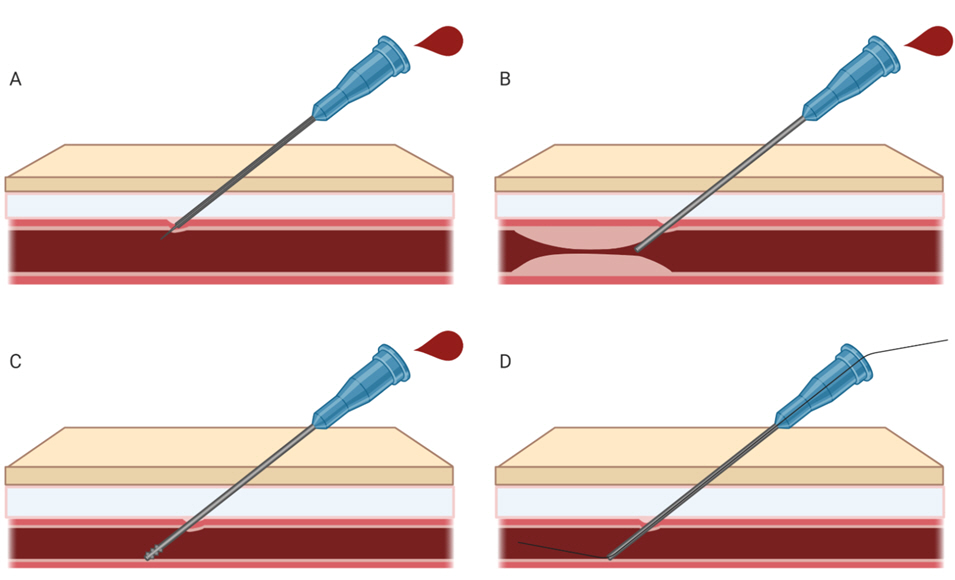
There are two steps of arterial cannulation: puncture of the vessel with a needle and insertion of the catheter after the puncture. Even after successful puncture, advancement of the catheter is difficult in some cases. Possible causes include a non-optimal location of the needle tip or catheter tip and vasospasm. In such cases, the guidewire technique is useful (Fig. 6). For radial artery cannulation in neonates and infants, guidewire-assisted radial artery cannulation was superior to the direct technique in terms of first-attempt success rate and overall success rate without an increase in procedure time [30]. The use of a guidewire also increases the success rates in critically ill patients [53,54].
4. Wrist, ankle, and leg position for cannulation
For radial artery cannulation, a recent meta-analysis showed that 45° of wrist extension, compared to the neutral position, increased the anterior-posterior diameter of the radial artery and facilitated radial artery cannulation by increasing the success rate and decreasing the procedure time in adults [55,56]. There are no data regarding the effect of ankle position on the diameter, depth, or success rate of arterial catheterization in the dorsalis pedis artery or posterior tibial artery in adults.
In pediatric patients, Kim et al. [8] reported the effect of wrist and ankle position on the diameter and depth of the radial, posterior tibial, and dorsalis pedis arteries. Wrist extension up to 45° decreased the depth of the radial artery without changes in diameter or cross-sectional area. For the posterior tibial artery, ankle dorsiflexion and eversion significantly decreased the depth of the posterior tibial artery from 5 mm to 4 mm from the skin, which could influence the success rate of posterior tibial arterial cannulation. For the dorsalis pedis artery, ankle plantar flexion decreased the cross-sectional area.
Overlapping of the common femoral artery and the femoral vein is observed in 65% of adults and 55% of pediatric patients [25,57]. Therefore, distinguishing the femoral artery and femoral vein is very important especially during the LAX approach. Arteriovenous fistula formation can occur after an inadvertent wall puncture between the femoral artery and femoral vein. In adults, external rotation and abduction of the leg (frog-leg position) [58] and a frog-leg position with a combination of back extension decreased the overlapping portion between the femoral artery and femoral vein [59]. In pediatric patients, leg abduction with a range between 48° and 58° and external hip rotation can minimize the overlap between the femoral artery and vein [60].
COMPLICATIONS AND PREVENTION
Complications rarely arise from peripheral arterial catheterization (21 complications after 62,626 arterial cannulations [0.03%]), including pulseless extremities, occluded arteries, and other vascular/neurologic findings [4]. However, complications associated with arterial catheterization are common in critically ill adults [61] and children [62]. Younger children, such as neonates and infants, have a higher risk of complications [5]. The overall complication rate was 32.1% in patients aged < 2 years. Among the complications, vasospasm and hematoma were found in 19.6% and 23.2% of patients, respectively, which could have been neglected if post-cannulation ultrasound evaluation was not done.
Furthermore, complications vary depending on the catheterization site. Recently, the overall major complication rate within 30 days was 0.034-0.2% in adults [4] and children [5], but the complication rate related to the femoral artery was 0.7-25% in children [5,22]. Site-specific complications are related to the anatomical characteristics of these arteries. Hence, the anatomy and relationship around the target artery must be understood well. An ultrasound-guided procedure is recommended to prevent possible complications.
Arterial occlusion or ischemia
Arterial occlusion or ischemia following cannulation is a typical complication [42]. Permanent ischemia is rare (0.09%), but temporary occlusion or ischemia is reported in up to 38% of cases depending on risk factors [2,63,64]. Therefore, caution should be exercised when patients have risk factors. Risk factors for overall vascular complications associated with catheterization in adults include the use of vasopressors, previous injury of the artery, longer duration of cannulation, hematoma, cardiac output reduction, female sex, a smaller diameter of the artery, and disseminated intravascular coagulation [63].
Vasospasm
Vasospasm can be caused by mechanical stimulation and damage to the endothelium of the vessel during arterial catheterization. This stimulation releases adenosine diphosphate and thromboxane A2, aggregating platelets and leading to vasospasm or even complete occlusion [64]. An old study reported that the incidence of vasospasm is up to 57% [2]. Vasospasm is more common in neonates or very small children because of low cardiac output, dehydration, and polycythemia [65]. Vasospasm may cause a discrepancy between peripheral arterial pressure and central arterial pressure in cardiac surgery with cardiopulmonary bypass [22], which may affect interpretation. Moreover, cannulation and catheter advancement can be disturbed by vasospasms [9,66,67]. Most vasospasms can be treated conservatively and completely recover. However, clinicians should always keep in mind that vasospasms can become progress to cause ischemia and necrosis.
Hematoma/bleeding
The reported incidence rates of major bleeding are 0.05% and 1.58-2.3% [4,64] for the radial and femoral arteries, respectively. Bleeding that is observed externally can be treated by applying pressure to the bleeding site directly, and thus can be easily controlled. The occurrence of hematomas related to arterial catheterization is reported to be 6.1-23.2% [9,60,64,68]. Fatal hematomas, such as retroperitoneal hematomas following femoral arterial cannulation, is rare (0.15%), but may require surgical intervention. Therefore, prevention is important. The incidence of such retroperitoneal hemorrhages can be reduced using ultrasonography [69].
Infection
The incidence rates of arterial catheter-associated infections and sepsis are reported to be 0.024-0.38% in adults [4,64] and 1.4% in children [5]. One meta-analysis revealed that the incidence of arterial catheter-related bloodstream infections was 0.7% [70]. However, the femoral artery (0.44%) was more associated with sepsis and infection than the radial artery (0.78%) [64]. Arterial catheter-related infections are associated with increased morbidity and mortality, and require immediate treatment [71]. Ten percent of local infections and colonization of arterial catheters can cause bacteremia, with the cause of 63% of arterial catheter-related bloodstream infections revealed be due to an extraluminal factor [72]. The risk factors related to catheter-related infections include patient factors such as chronic cardiac failure, chronic respiratory failure, immune deficiency, and diabetes, as well as procedural factors, including duration of catheter placement, bacteria-compatible catheter type, and antibiotic bonding [71].
The risk of infection when using ultrasound is controversial. In terms of reducing the attempt number and time when using ultrasound, the use of ultrasound during arterial cannulation may prevent infection [28]. On the contrary, some argue that the use of the gel for a better view of ultrasound could increase infection risk [33]. However, a recent large randomized controlled trial demonstrated that the infection risk of arterial cannulation using ultrasound did not increase compared to that without ultrasound [43].
Nerve injury
Neurological problems related to catheterization can vary depending on the site of arterial cannulation [73]. The most vulnerable nerves are the ulnar nerve around the ulnar artery, the median nerve around the brachial artery, the femoral nerve around the femoral artery, the posterior tibial nerve around the posterior tibial artery, and the deep peroneal nerve around the dorsalis pedis artery. These nerves can be easily injured directly by the needle or the pressure following hematoma, pseudoaneurysm or fluid extravasation, and chemical injury [74]. The reported incidence of nerve injury varies, but median nerve damage related to brachial arterial cannulation is most common at 9%, followed by femoral nerve injury [73]. With ultrasound guidance, the anatomical relationship between the target artery and adjacent structures can be evaluated before cannulation, and the direction of the needle can be adjusted to avoid direct trauma to the nerve during arterial catheterization [73].
CONCLUSION
Ultrasound-guided arterial catheterization is more effective than conventional methods in terms of success rate and complications. For successful ultrasound-guided arterial catheterization, it is necessary to select an appropriate artery and catheter, perform an accurate ultrasound-guided procedure, and apply useful techniques to increase success rates. Practitioners should become familiar with vascular anatomy and ultrasound-guided arterial catheterization techniques.