Comparison of prophylactic effect of topical Alchemilla vulgaris in glycerine versus that of dexamethasone on postoperative sore throat after tracheal intubation using a double-lumen endobronchial tube: a randomized controlled study
Article information

Abstract
Background
Sore throat and hoarseness frequently occur following general anesthesia with tracheal intubation and are effectively reduced when dexamethasone is used prophylactically. Alchemilla vulgaris in glycerine (Neo Mucosal Activator®) suppresses inflammatory response, possibly relieving sore throat.
Methods
We enrolled 94 patients (age ≥ 18 years) scheduled for thoracic surgery using double-lumen tube intubation. Before intubation, 0.2 mg/kg of dexamethasone was administered intravenously and 2 ml of normal saline was sprayed into the oropharyngeal cavity (Group D; n = 45), or 0.04 ml/kg normal saline was administered intravenously and 1 g of Neo Mucosal Activator® mixed with 1 ml of normal saline was sprayed into the oropharyngeal cavity (Group N; n = 43), in a double blind and prospectively randomized manner. Postoperative sore throat and hoarseness were recorded using a numeral rating scale and a 4-point scale to detect a change in voice quality following tracheal extubation (at 1, 6, and 24 h). The primary outcome was the incidence of sore throat at 24 h following surgery. The secondary outcomes were incidence and severity of sore throat and hoarseness.
Results
There were no significant differences in the incidence of sore throat at 24 h following surgery (57.8% vs. 46.5%; P = 0.290) or in the incidence and intensity of sore throat and hoarseness at 1, 6, and 24 h following surgery between the groups.
Conclusions
A. vulgaris in glycerine did not significantly differ from dexamethasone for preventing sore throat and hoarseness owing to intubation.
INTRODUCTION
Sore throat and hoarseness are common complications of general anesthesia. These complications present in approximately 62% of patients as a result of mucosal damage that occurs during the insertion of a laryngoscope into the oropharynx and/or mucosal damage due to upper airway irritation by the intubated tube. An intubated tube can cause inflammatory reactions in the airways, mucosal thickening, and, consequently, sore throat, which lowers postoperative patient satisfaction. The risk factors for sore throat and hoarseness include sex (female), age (young), pre-existing lung disease, prolonged duration of anesthesia, intubation without neuromuscular blockade, use of double-lumen tubes, and high tracheal tube cuff pressures [1].
The double-lumen endobronchial tube (DLT) is used in video-assisted thoracoscopic surgery requiring one-lung ventilation as it is quicker and more effective than bronchial blockers for lung isolation. However, owing to their large diameters, DLTs frequently cause sore throat and hoarseness for up to two weeks following treatment of airway injuries such as vocal cord hematoma and bronchial edema, thereby significantly increasing patient discomfort [2,3].
Intravenous dexamethasone is prophylactically used to prevent the sore throat and hoarseness that occur after general anesthesia owing to airway intubation [1,4–7]. However, the potential side effects of dexamethasone limit its use in patients for whom steroid use is contraindicated. In a study by Shrivastava and John [8], Alchemilla vulgaris in glycerine (AVG), also called Lady’s Mantle, which has traditionally been used for oral hygiene, induced complete healing in 75% of patients within 2–3 days after topical application of 2–3 drops three times a day to minor oral ulcers. In the present study, for the first one, we aimed to investigate the preemptive effects of spraying AVG into the oropharynx to prevent sore throat resulting from intubation for general anesthesia.
MATERIALS AND METHODS
This study was approved by the Institutional Review Board of Dong-A University Hospital (no. DAUHIRB-18-195) and registered in the CRIS (no. KCT0003842). Of the patients scheduled for elective surgery using a DLT between October 2018 and May 2020, those who were deemed appropriate for participation and who had given written consent were included in this study. Ninety-four patients with American Society of Anesthesiologists physical status I–III, aged 18 years or older, were enrolled in this study.
The exclusion criteria were as follows: 1) Patients who were receiving steroid-containing medications; 2) patients who were allergic to honey (because honey is a component of Neo Mucosal Activator®) or Neo Mucosal Activator® (a topical application of AVG); 3) patients with diagnosed or suspected malignancy; 4) patients scheduled for pneumonectomy; 5) patients who showed signs of infection of the upper airway or had sore throat or hoarseness; and 6) patients who had uncontrolled diabetes. Reasons for withdrawal were as follows: 1) Duration of tracheal intubation > 300 min or < 60 min; 2) DLT failure; and 3) extubation not performed owing to the requirement of continuous mechanical lung ventilation after surgery.
Before being transferred to the operation room, the patients were randomly assigned to one of two groups according to a computer-generated random number table. The medications to be used in each procedure were placed in 5-ml syringes and 2-ml spray bottles (Fig. 1) by a researcher who was not responsible for performing anesthesia or collecting data, and these medications were handed over to a blinded anesthetic nurse. In the experimental group (Group N), normal saline was intravenously administered at 0.04 ml/kg, and 1 g of AVG (Neo Mucosal Activator®, DAEUN Medical, Korea) was mixed with 1 ml of normal saline and sprayed into the oropharyngeal cavity around the vocal cords. In the control group (Group D), dexamethasone was intravenously administered at 0.2 mg/kg, and 2 ml of normal saline was sprayed into the oropharyngeal cavity around the vocal cords. As the mixed solution and dexamethasone were both transparent and not easily distinguished from normal saline, we did not cover the solutions.

A 2 ml spray bottle.
Anesthesia was induced by two senior residents blinded to the medication used. Patients were intramuscularly injected with glycopyrrolate (0.2 mg) and intravenously injected with famotidine (20 mg) before surgery and placed under standard monitoring after entering the operating room. General anesthesia was induced by the intravenous administration of propofol (2.0 mg/kg) and rocuronium (0.6–0.9 mg/kg) as a neuromuscular blocking agent while monitoring the bispectral index (BIS) (Aspect Medical Systems, USA).
The medication in the 5-ml syringe was intravenously administered immediately following rocuronium administration. After achieving sufficient neuromuscular blockade following bag mask ventilation (train-of-four [TOF] count 0), the medication in the spray bottle was sprayed into the oropharyngeal cavity using a video laryngoscope (C-MAC, KARL STORZ-ENDOSKOPE, Germany). A DLT (Shiley, Covidien, Ireland) was then inserted: 35-Fr tubes were used for females and 37-Fr tubes for males. If the original tube could not be inserted, the original tube was substituted for a smaller tube; 32-Fr and 35-Fr tubes were used for females and males, respectively. After locating the DLT by auscultation, fiberoptic bronchoscopy (external diameter 3.1 mm, Olympus Optical, Japan) was used to adjust the insertion depth, and the depth was reassessed after placing the patient in a lateral position. Anesthesia was maintained with sevoflurane concentrations of 1.5–2.5 vol% to maintain a BIS of 40–60. Remifentanil infusion (0.05–2 μg/kg/min) was administered for pain control. Vecuronium (0.01 mg/kg) was administered at a TOF count of 1 to maintain deep neuromuscular blockade. Intracuff pressure was maintained at 15–25 cmH2O using a cuff pressure manometer (Cuff Pressure Gauge, VBM Medizintechnik, Germany).
At the end of the surgery, fentanyl (30 μg/kg) and ramosetron (0.6 mg) were mixed with normal saline in a total volume of 100 ml in a patient-controlled analgesia (PCA) infusion system (GemStarTM Infusion System, Hospira, Inc., USA), and the system was connected to the patient. The continuous infusion rate was set to 1 ml/h, and the bolus dose to 1 ml (10-min lockout time).
After the surgery was complete, tracheal suctioning was gently performed, and sugammadex was injected at 2 mg/kg for inducing a moderate neuromuscular block (at least one twitch in a TOF) and at 4 mg/kg for inducing a deep block (no twitches in a TOF). After the TOF ratio reached > 0.9, the patients could breathe on their own; following instructions, oral secretions were suctioned again, and the patient was extubated [9].
The primary outcome was the incidence of sore throat at 24 h after surgery. The secondary outcomes were the incidence and the severity of sore throat and hoarseness. Following surgery, the patients rated the severity of sore throat on a numeric rating scale (NRS) and the severity of hoarseness as none, mild, moderate, and severe (based on vocal changes at 1, 6, and 24 h after surgery). In addition, the incidence of sore throat was determined as NRS ≥ 1. The patients were also asked to record any side effects (e.g., allergic reaction, nausea, vomiting). Postoperative use of analgesics and side effects were checked by reviewing medical records. The collected data were reviewed with respect to the enrollment number assigned to each patient.
Statistical analyses
A pilot study was conducted on 30 patients (15 patients per group) to determine the required sample size. Two patients in Group D and three patients in Group N were excluded from this study. Sore throat was observed in 7/13 (53.8%) patients in Group D and 3/12 (25%) patients in Group N at 24 h after surgery. The results of the power analysis indicated a minimum requirement of 42 patients in each group (β = 0.2 and α = 0.05). To compensate for potential dropouts (10%), we selected a sample size of 47 patients per group.
Mean ± standard deviation or number (%) are presented for each variable. The chi-square test with Fisher’s exact test was used for categorical data. The Student’s t-test was used to analyze continuous data. Repeated measures analysis of variance (ANOVA) was used for time-group analysis. Two-tailed P values were calculated, and the level of significance was set at P < 0.05. All analyses were performed using SPSS Statistics 26 software (IBM Corp., USA).
RESULTS
In total, 6 of the 94 patients enrolled in this study were excluded: 2 patients in Group D and 3 patients in Group N whose intubation time exceeded 300 min, and 1 patient in Group N for whom extubation was not performed owing to postoperative ventilation care (Fig. 2). Table 1 shows the characteristics of the final patient groups. No significant differences were observed in the factors that affect postoperative sore throat and hoarseness, including duration of tracheal intubation and operation time, number of intubation attempts, and time to achieve intubation (Table 2).
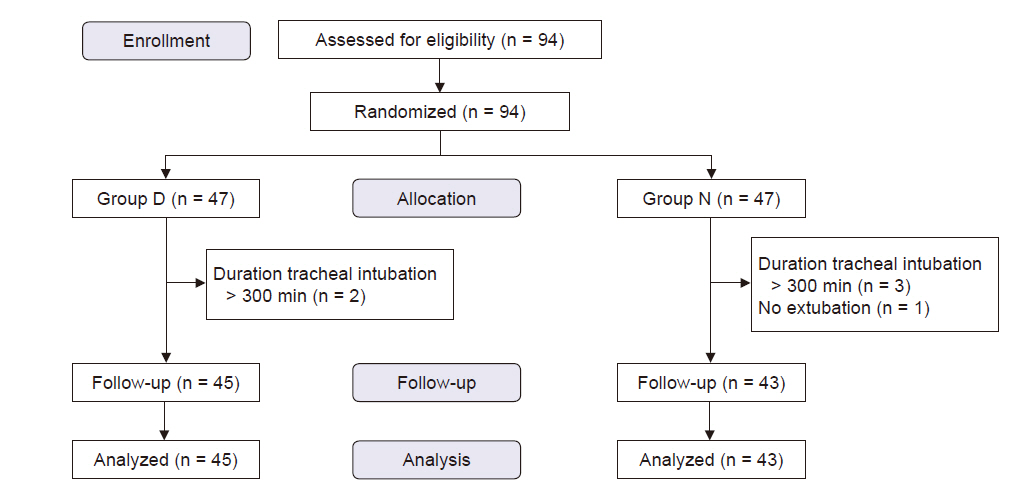
CONSORT flow chart for the study patients. Group D: dexamethasone group, Group N: Neo Mucosal Activator group.
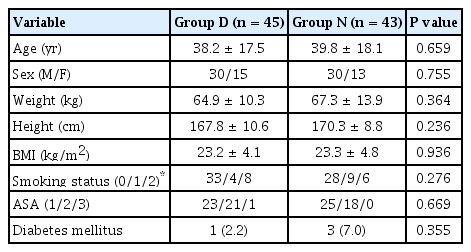
Patient Characteristics

Anesthetic Data
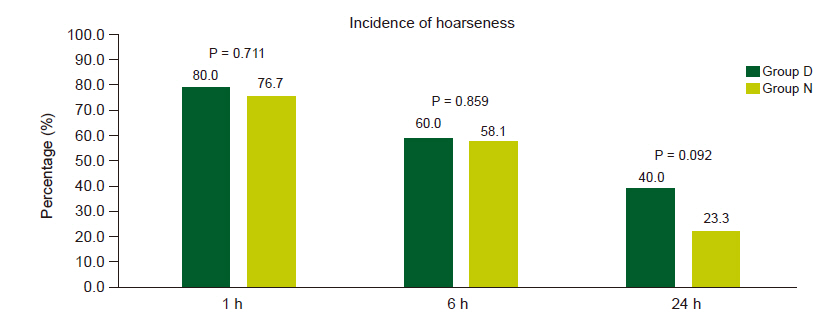
No significant difference in the incidence of sore throat at 24 h after surgery was observed between the two groups (57.8% vs. 46.5%; P = 0.290) (Fig. 3). No significant difference in the incidence of sore throat (Fig. 3) and incidence (Fig. 4) and severity (Table 3) of hoarseness was observed between the two groups at any time point. No significant differences in the intensity of sore throat at 1, 6, and 24 h post-surgery were observed between the groups (Fig. 5). A repeated measures ANOVA showed a reduction in intensity over time in each group (both P < 0.001), but no significant difference between groups (P = 0.273) (Fig. 5).
Incidence of sore throat at follow-up (1, 6, and 24 h). Group D: dexamethasone group, Group N: Neo Mucosal Activator group.
Incidence of hoarseness at follow-up (1, 6, and 24 h). Group D: dexamethasone, Group N: Neo Mucosal Activator group.
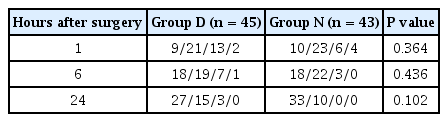
Severity Score of Hoarseness
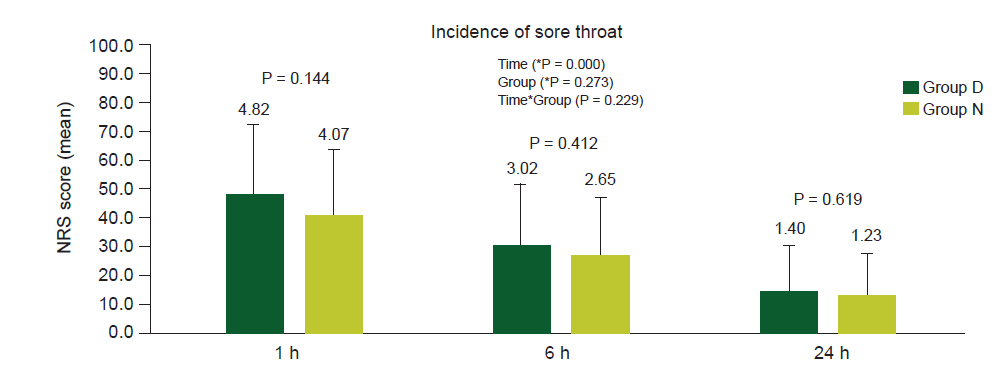
Intensity of sore throat at follow-up (1, 6, and 24 h). Values are presented as mean ± SD. Group D: dexamethasone, Group N: Neo Mucosal Activator group, NRS: numeric rating scale. *P value was obtained by repeated measure ANOVA.
Additionally, the number of patients receiving non-steroidal anti-inflammatory drugs (NSAIDs) for postoperative pain control in group D was lower than in group N (42.2% vs. 65.1%; P = 0.031). No significant differences were observed in the amounts of morphine required and pain buster (Pain Relief System, Halyard Health, Inc., USA) used between the groups (Table 4).
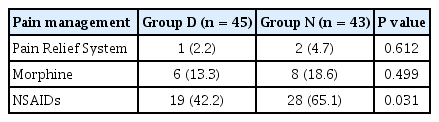
Postoperative Analgesia
DISCUSSION
Several studies [1,4–7,10–12] have been conducted to test methods that prevent the sore throat and hoarseness that occur after intubation for general anesthesia. Dexamethasone, which is commonly prescribed for sore throat caused by tracheal mechanical irritation, inhibits leukocyte migration, cytokine secretion, and fibroblast proliferation to reduce inflammatory reactions caused by tissue damage [1,4,7]. Park et al. [5] reported that a prophylactic administration of 0.2 mg/kg dexamethasone effectively reduces the incidence and severity of sore throat and hoarseness. However, its use in immunosuppressed patients or patients with uncontrolled diabetes is limited, as the side effects of dexamethasone include hyperglycemia, peptic ulcer, increased susceptibility to infection, delayed wound healing, and adrenal suppression [5].
According to Yang et al. [10], spraying 5% ketorolac tromethamine, an NSAID, into the endotracheal tube reduces the incidence of sore throat following intubation. Similar effects have been observed in studies in which benzydamine hydrochloride is sprayed into the oropharyngeal cavity and an endotracheal tube [11,12]. Benzydamine hydrochloride reduces pain through its anti-inflammatory and analgesic mechanisms of action. However, benzydamine hydrochloride can also cause side effects such as local numbness, a burning sensation, nausea or vomiting, cough, and dry mouth [11].
In an effort to prevent sore throat resulting from intubation (while avoiding the side effects of known treatments), we have investigated the effects of Lady’s Mantle on the oropharyngeal cavity. Lady’s Mantle is an anti-inflammatory folk medicine from Europe derived from A. vulgaris. In our study, AVG did not significantly reduce the incidence of sore throat compared to dexamethasone. However, there was no significant difference in the incidence and severity of sore throat and hoarseness observed over time between AVG and intravenously administered dexamethasone. A. vulgaris promotes the proliferation of macrophages and lymphatic vessels and the migration of keratinocytes, fibroblasts, and endothelial cells, thereby promoting wound healing. Glycerine, which is hypertonic, causes the exudates in the wound to move toward the mucosal layer by osmosis and thus removes bacteria [8,13,14]. Therefore, AVG sprayed into the oropharyngeal cavity may promote mucosal healing and prevent infection (as do dexamethasone and NSAIDs when sprayed into the oropharyngeal cavity), consequently reducing the incidence of sore throat and hoarseness.
To reduce the risk of sore throat, we attempted to reduce trauma to the glottis using a videoscope instead of a direct laryngoscope; the laryngoscope applies forward and upward forces to align the visual, oral, pharyngeal, and laryngeal axes and thus can damage arytenoid cartilages and mucosa [15]. In addition, we maintained the cuff pressure at 15–25 cmH2O to reduce direct trauma to the tracheal mucosa [1]. It is possible that these actions might have contributed to the insignificant statistical difference between the two groups.
The increase in the incidence rate in this study could be mainly attributed to the fact that the incidence of sore throat was determined as NRS ≥ 1. In a previous study that examined the NRS pain score of patients and the need for additional opioids after surgery [16], the NRS cut-off point was set as 1, and the sensitivity and specificity were 98% and 20%, respectively. The positive predictive value was 11%, and thus it could be assumed that a very low percentage of patients complained of pain that required rescue analgesia. In our study, while the incidence rate was high (Fig. 3), the intensity was not severe (Fig. 5). In addition, among the factors that may have affected the patients’ perspectives on rating pain, the patient's desire to confirm his or her pain from professionals may have caused them to record low scores [17]. In addition, tracheal intubation was performed by senior residents who did not have a high level of experience; although a previous study reported no significant difference in performance between consultants and trainees [1], this may have contributed to the high incidence. All patients were subjected to PCA after surgery and reported the common side effects of general anesthesia or opioid use including nausea, vomiting, and dizziness (n = 4, 2, 2, respectively). No allergic reactions, adverse drug reactions, or hyperglycemia occurred. In addition, side effects associated with NSAID treatment, including numbness, burning or stinging sensation, cough, dry mouth, thirst, or headache, were not reported [11]. Comparison of pain control between the groups showed that the patients in Group D required lesser NSAIDS than those in Group N (42.2% vs. 65.1%; P = 0.031). Although we did not evaluate postoperative surgical site pain and total opioids consumption in this study, other studies have reported that these may be related to the systemic effect of intermediate-dose dexamethasone (0.11–0.2 mg/kg) [18,19].
This study has several limitations. First, because we did not include a control group that did not receive prophylactic medication, we could not determine the extent to which AVG reduced the incidence of sore throat. Second, as AVG was prepared as a colloid by mixing normal saline with Neo Mucosal Activator® to reduce the risk of aspiration because of its viscous property, the effect of spraying normal saline on the laryngeal area remains unknown. Furthermore, as patients with sore throat or hoarseness were not examined with a laryngoscope, we could not assess them for laryngitis or vocal cord injury.
In conclusion, spraying AVG into the oropharynx did not have a significantly different effect in preventing sore throat and hoarseness owing to intubation when compared with that achieved by intravenous injection of low-dose dexamethasone. Further research is warranted on the method of application and optimal dose of AVG through a comparison with a placebo and other medications, and to verify the preemptive effect of AVG against the sore throat and hoarseness that occur after intubation for general anesthesia.
Acknowledgements
This study was supported by Dong-A University.
Notes
CONFLICTS OF INTEREST
No potential conflict of interest relevant to this article was reported.
DATA AVAILABILITY STATEMENT
The data that support the findings of this study are available from Dong-A University but restrictions apply to the availability of these data, which were used under license for the current study, and so are not publicly available. Data are however available from the authors upon reasonable request and with permission of Dong-A University.
AUTHOR CONTRIBUTIONS
Conceptualization: So Ron Choi. Data curation: Seong Yeop Jeong, Joon Ho Jeong, Sung Wan Kim, Kyung Hyun Lee. Formal analysis: Chan Jong Chung, Seong Yeop Jeong, Sung Wan Kim, Sang Yoong Park. Methodology: Chan Jong Chung, Seong Yeop Jeong, Jeong Ho Kim, Sang Yoong Park, So Ron Choi. Project administration: Seong Yeop Jeong, Joon Ho Jeong, Sung Wan Kim, Kyung Hyun Lee. Visualization: Jeong Ho Kim, Sang Yoong Park. Writing - original draft: Seong Yeop Jeong. Writing - review & editing: Chan Jong Chung, Seong Yeop Jeong, Jeong Ho Kim, Sang Yoong Park. Investigation: Chan Jong Chung, Seong Yeop Jeong, So Ron Choi. Resources: Joon Ho Jeong, Kyung Hyun Lee. Supervision: Chan Jong Chung, Sang Yoong Park, So Ron Choi.