INTRODUCTION
Ultrasound-guided interfascial plane blocks are commonly used to provide postoperative analgesia in different anatomical regions [1]. Among the interfascial blocks, the quadratus lumborum block (QLB) is a field block used for analgesia after abdominal surgery [2,3]. This block, which was later used in different anatomical regions (hip surgery, lower limb vascular surgery, total hip arthroplasty, etc.) for analgesia in addition to the abdominal area, is performed by injecting a local anesthetic (LA) between different fascial layers according to the anatomical position of the thoracolumbar fascia (TLF) and quadratus lumborum (QL) muscle [3]. In the anterior QLB (aQLB), the LA is injected between the psoas and QL muscles. Different mechanisms of action of the aQLB have been proposed in case reports and clinical trials. With aQLB, analgesia can be achieved between the 6th thoracic and 2nd lumbar dermatomes [2]. Although the primary goal is to block the thoracolumbar nerves, paravertebral spread of the LA and sensory innervation in the TLF may be involved in the mechanism of action [2,4]. TLF is an anatomical formation consisting of aponeurotic and fascial layers that separate the paraspinal muscles in the lumbar region from the muscles of the posterior abdominal wall. It is a part of the myofascial structure surrounding the erector spinae, QL, and psoas muscles in the posterior and lateral lumbar regions with aponeuroses of the abdominal wall muscles. It plays a major role in stabilizing the lumbar spine and load transfer. In addition, it carries both proprioceptive and nociceptive innervations and may be sensitive; however, the evidence is weak [5]. The relationship between the TLF and anterior abdominal wall muscles has been demonstrated in different studies. The intra-abdominal pressure and muscle structure may affect the TLF. The connection of the TLF with other anatomical structures may affect the outcomes of blocks administered in the TLF.
The aim of the present study was to test the hypothesis that pressure changes between the aQLB and middle TLF layers influenced the sensory block level.
MATERIALS AND METHODS
Patient selection
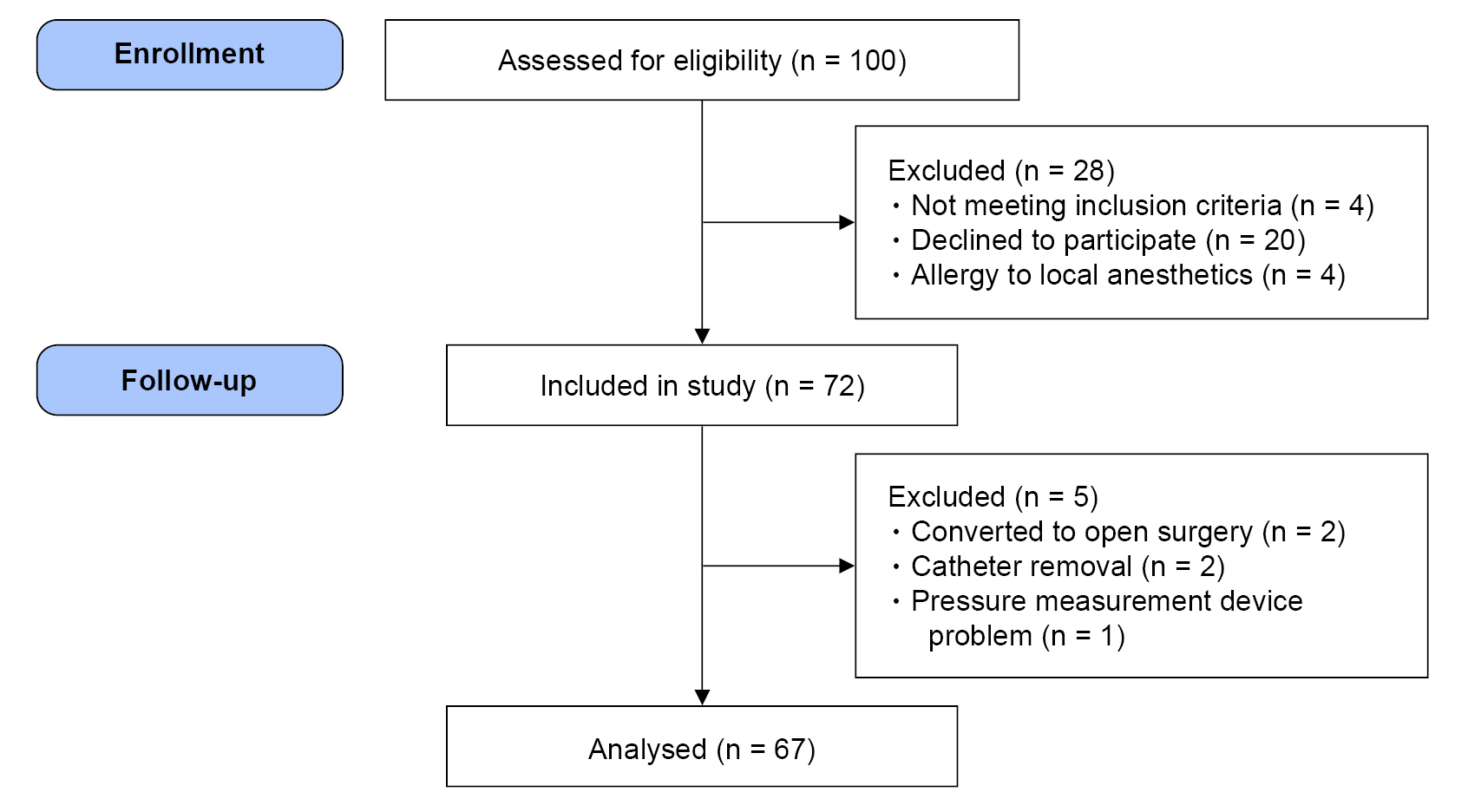
A total of 100 patients scheduled to undergo laparoscopic cholecystectomy were evaluated in this prospective observational study following Institutional Ethics Committee (IEC) approval and registration of the clinical trial records (IEC number: 2019-5/26; ClinicalTrials.gov identifier: NCT04094987). All patients provided written informed consent for participation in the study. This study was conducted in accordance with the principles of the Declaration of Helsinki. Inclusion criteria were: laparoscopic cholecystectomy, age of 18-65 years, American Society of Anesthesiologist grade I-III, and informed consent. Exclusion criteria were: allergy to LA, previous opioid use, uncontrolled diabetes mellitus, hypertension, and the presence of infection at the site of application. Finally, a total of 72 patients were included in this study (Fig. 1).
Anesthetic management
Propofol, rocuronium bromide, and fentanyl citrate were intravenously administered to induce anesthesia. A mixture of sevoflurane, air, and O2 was used at a flow of 2.5-3 L/min to maintain anesthesia. Mechanical ventilation was applied, providing an 8 ml/kg tidal volume in a volume-controlled mode. The intraoperative CO2 levels were monitored using the end-tidal CO2 module values of the anesthesia machine. Rocuronium bromide (0.6 mg/kg) was used as the neuromuscular blocking agent. A train of four monitor was used for neuromuscular monitoring. When the TOF ratio had reached 25%, rocuronium bromide was added at the rate of ¼ of the intubation dose. A single dose of a nonsteroidal anti-inflammatory drug (tenoxicam 20 mg, intravenously) was administered 15 min before the end of the operation, and a tramadol + saline solution (5 mg/ml) was prepared for the postoperative patient-controlled analgesia (PCA) protocol. The PCA device was set with no basal infusion, a lockout time of 30 min, and a demand dose of 25 mg.
Anterior quadratus lumborum block
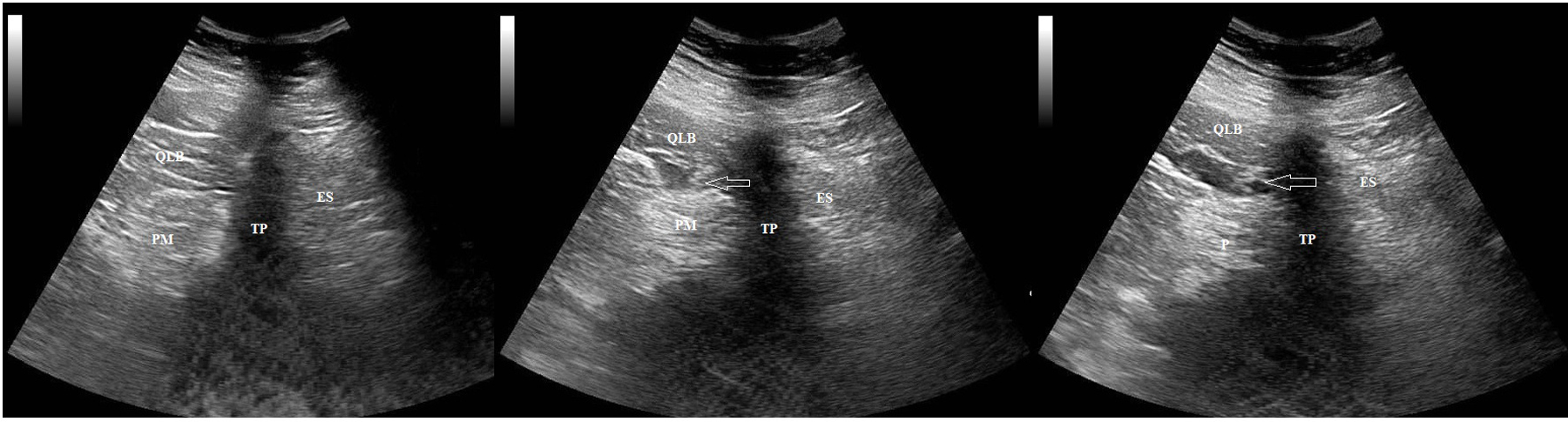
The aQLB was applied preoperatively 30 min before induction of anesthesia in the lateral decubitus position bilaterally. A convex ultrasound probe (2-6 MHz MyLab30, Esaote) was placed on the iliac crest, transverse to the axillary line, and the shamrock sign was defined by the posterior guided probe at the level of the L4 vertebra, which comprises the L4 vertebral body, transverse process, and QL, psoas, and erector spinae muscles. A peripheral nerve block was administered with a 100-mm, 18-gauge Tuohy needle (SonoPlex Pajunk) directed to the anterior TLF between the QL and psoas muscles [2,6]. A 20-gauge catheter with a central opening was placed after the location had been confirmed by hydrodissection using 3 ml saline (Fig. 2). After the preoperative pressure measurement, a total of 50 ml of 0.25% bupivacaine was injected, with 25 ml on the right and left sides.
Interfascial pressure (IFPs) measurement
The transducer line of the disposable pressure measurement set was connected to a catheter using a T-connector. A pressure-measuring transducer was secured in the region of block application and connected to the monitor. The pressure transducer was fixed at the same height as the block application area and connected to a monitor. The transducer was set at this altitude at the zero level. IFPs was measured after a 5 ml saline injection, with the patient in the supine position. Changes in the respiratory pressure were also detected (Fig. 3). Over 1 min, three measurements (average inspiratory and expiratory values for each measurement) were made, and the average of these measurements was recorded. All measurements were performed according to the standard protocols. The level of bilateral sensory blockade was monitored using a cold test 30 min after the block application and 30 min after the end of the operation.
Outcome measures
The primary outcome measure was the correlations of the IFPs (mmHg) during block application, 30 min intraoperatively, and 30 min postoperatively with the level of the sensory block. The secondary outcome measure was the sensory block level 30 min after block application and 30 min postoperatively determined using the cold test. Visual analog scale (VAS) scores were obtained 30 min and 6, 12, and 24 h postoperatively, and the amount of 24 h tramadol consumption was measured.
Statistical analysis
Descriptive statistical techniques and chi-square (χ2) tests were used to compare qualitative data. The Shapiro-Wilk test was used to evaluate the normality of data distribution. The data distribution was not normal. The Wilcoxon signed-rank test was used to analyze repetitive measurements. Spearman’s rho correlation test was used to evaluate correlations. An association was considered significant at a P-value < 0.05. Statistical software SPSS Version 22.0 (IBM Co.) was used for the statistical analyses.
Power analysis
The correlation coefficient of the pressure and block level was an r of 0.335 in the pilot study, including 10 patients. The necessary sample size was determined as 64 patients in order to obtain an 85% (α = 0.05) study power. A total of 72 patients were included in the study, considering the possible setbacks. G* power (ver. 3.1.9.4, University of Kiel) was used for sample size calculation [7].
RESULTS
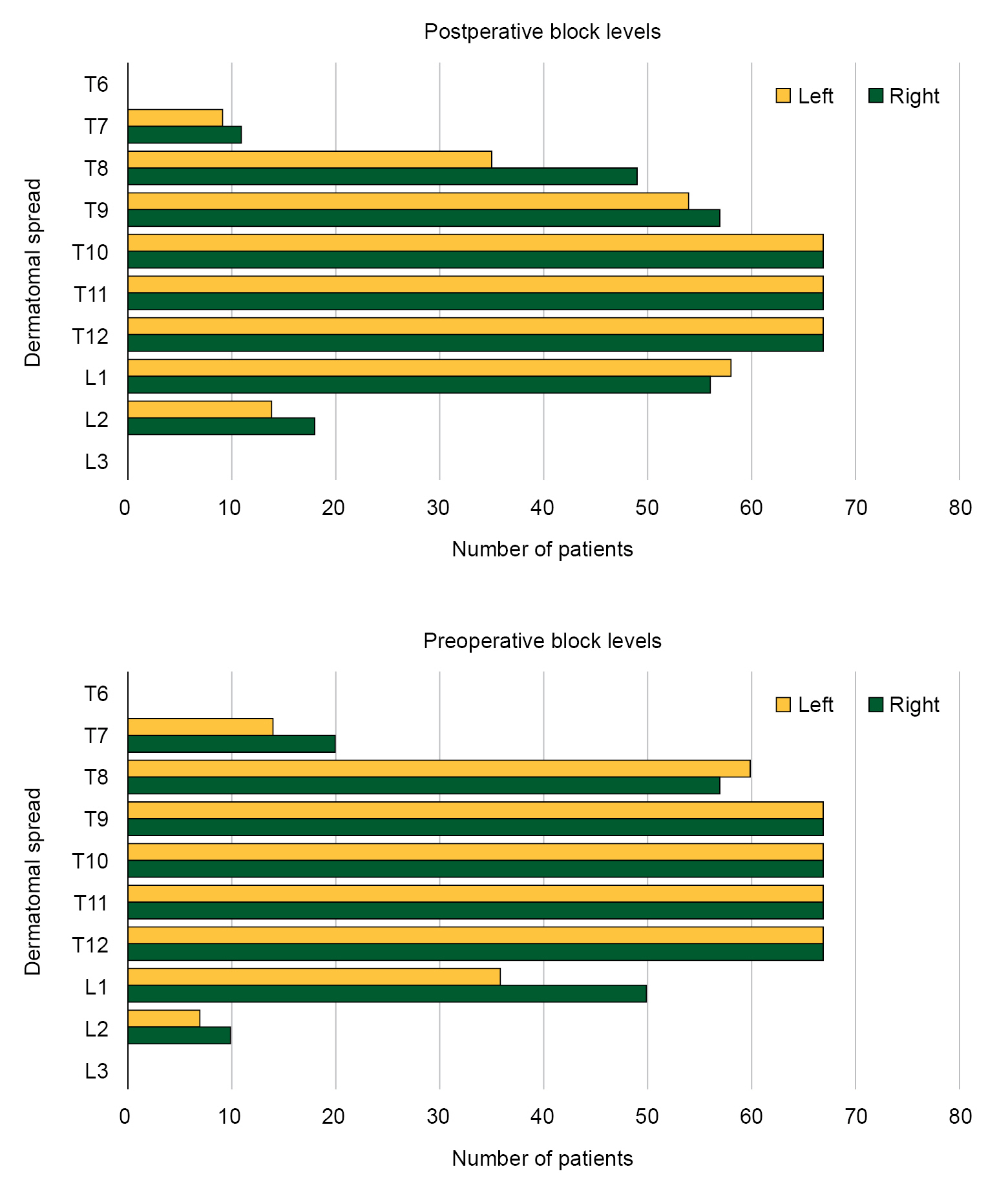
A total of 72 patients were included in the study. However, the study was completed with only 67 patients owing to conversion to open surgery in two patients, accidental catheter removal in two patients, and a problem with the pressure measuring device in one patient (Fig. 1). Table 1 shows the demographics of the patients who completed the study. Fig. 4 shows the distribution of the sensory blockade 30 min after block application as right- and left-sided block levels. In the interfascial area, the preoperatively and intraoperatively measured IFPs differed significantly between the right and left sides (P < 0.05; Table 2). The preoperative and postoperative block levels showed significant differences between the right and left sides (P < 0.05; Table 2). A weakly negative correlation (right: r = 0.374; left: r = 0.470) was found between the block levels obtained preoperatively and postoperatively and the preoperatively measured IFPs, while no correlation was found with the intraoperative or postoperative IFPs (Table 3). The body mass index (BMI) values of the patients did not correlate with the measured block levels. A weakly positive correlation was found between BMI and IFPs measured during the preoperative, intraoperative, and postoperative periods (Table 3). In the multiple regression analysis applied to determine the effect of IFPs and BMI together on block levels, no relationship was found with BMI, which may be owing to regulatory factors and the block levels (B: -0.68; 95% confidence interval: -0.258 to 0.122; r2 = 0.209; P = 0.477). The mean duration between the preoperative sensory block measurement time and the postoperative sensory block measurement time was 177.8 ± 11.1 min. The decrease in the sensory block level between the two measurement times was 4% (minimum: -42.86; maximum: 0.00). A negligible correlation was found between the sensory block level change and baseline IFPs (r = 0.114). The mean VAS scores measured at 2, 6, 12, and 24 h postoperatively were 1.14 ± 0.97, 1.07 ± 0.89, 1.28 ± 1.15, and 1.28 ± 1.15, respectively.
The mean total tramadol consumption of 24 h was 59.39 ± 46.2 mg. A negligible correlation was found between preoperatively measured IFPs and block levels, VAS scores, and tramadol consumption amount (r = 0.15). A negligible correlation was found between preoperative IFPs and block levels and tramadol consumption amount (r = 0.093).
DISCUSSION
We investigated the effect of pressure values measured using a catheter placed between the QL and psoas muscles in the anterior layer of the TFL at the block level and found a weakly negative correlation between the pressure values obtained from the measurements and the sensory block levels obtained 30 min after the block.
Two possible mechanisms of fascial plane blocks have been proposed, although they are yet to be fully confirmed. The first is a localized effect on the neurons and nociceptors at the injection site, which is mediated by bulk flow and diffusion processes. The second is the vascular absorption of LAs. Mass flow and diffusion are bulk flows in which the fluid is moved by pressure. The shape and limits of this mass flow are determined by the speed and direction of the injection, elastic recoil of the swollen fascial plane, and physical forces generated by muscle contraction and movement. This theory is supported by the finding of different levels of sensory blockade after block application at similar drug doses. Data are lacking in the literature regarding the exact definitions of these physical forces and their effectiveness. This study was aimed at quantifying the differences in pressure between the leaves of the TLF and their effects on the distribution of LAs. Therefore, the anatomical structure of the TLF is important [8].
The TLF contains three layers: posterior, middle, and anterior. While the posterior layer surrounds the erector spinae muscles, the middle layer is located between the erector spinae and the QL muscles. The anterior layer is located between the psoas and QL muscles [5]. QLB can be performed in four ways according to the anatomical structures defined in the three-layered model. If an LA is administered between the QL and psoas muscles, it is called QLB 3 (anterior); if it is administered between the QL and erector spinae muscles, it is called QLB2 (posterior); if it is administered lateral to the QL muscle, it is called QLB 1 (lateral); and if it is administered into the QL muscle, it is called muscular QLB [2]. Studies have investigated using the QLB to provide analgesia after surgeries, such as abdominal surgery (urological and laparoscopic surgeries), hip surgery, and cesarean section [2,3]. Different views have been reported regarding the effectiveness and mechanism of action of QLB in different studies. The amount of LA used and injection points of the same block vary in the literature [9-12]. In their systematic review and meta-analysis of these studies, Uppal et al. [3] reported the requirement of more studies to better characterize the risks and benefits associated with QLB. Studies on the mechanism of action of QLB have attempted to determine the extent of spread of the administered LAs. Paravertebral spread, which is a mechanism of action of QLB, other than blocking the thoracolumbar nerves, has been explored [2,3]. The distribution of LAs determined in cadaver studies has yielded different results [13-16].
While paravertebral spread was not found in two studies using 20 ml of dye, a study by Dam et al. [15] found dye spread in the paravertebral region and at the T9-T10 level [13-15]. In addition to the paravertebral spread of the administered dye, another study found spread up to the 7th thoracic level [16]. Another study attempting to determine the correlation between dermatomal spread and a cadaveric study in a case series found that the contrast agent diffusion area in the cadaver was consistent with sensory block levels in the case series. This study found the possibility of thoracic spread of the contrast agent and reported that the injected LA might follow the path of least resistance and prefer the fascia transversalis and transversus abdominis paths instead of the tight fascial compartments in the psoas major muscle [17]. In their case reports, Diwan et al. evaluated the diffusion of a contrast agent administered via a catheter in patients who had received QLB and had a catheter in the same area [18]. They reported that different blocks performed in the subcostal and iliac crest regions might change the paravertebral spread and that the resistance encountered during the procedure, injection rate, and LA volume might be associated with the block level [18]. In addition, they detected swelling in the anterior TLF layer on computed tomography after LA injection and stated that excessive pressure could damage the fascia [18].
Our results demonstrated a correlation between IFPs measured between the fasciae and sensory block levels, similar to previous studies. Our results suggest that IFPs between the fasciae may be a factor affecting the sensory level obtained after the QLB [17,18]. Various studies have found that the TLF is associated with the anterior abdominal wall muscles. A positive correlation was found between the increase in spinal stiffness and the extent of the increase in intra-abdominal pressure. Furthermore, they emphasized that it was impossible to determine whether the cause of the spinal stiffness was increased intra-abdominal pressure or abdominal muscle activity, although with inconsistent results [19,20]. IFPs during pneumoperitoneum creation for laparoscopy in the present study were higher than the initial measurements. This result is similar to that of other studies investigating the correlation of this change with increased intra-abdominal pressure, paraspinal muscles, and TLF [19,20].
This study has some limitations. First, intra-abdominal pressure was not measured during IFPs measurements. Second, sensory block levels were not monitored during the 24-h postoperative follow-up. Third, the injection pressure was not standardized during the drug injection in block application. Finally, we did not evaluate other pathologies (lumbovertebral pathologies or diseases that might cause back pain) that could alter the anatomical structure between the paraspinal muscles and fascia [21,22].
In conclusion, aQLB outcomes depend on multiple variables, such as needle direction, injection site, and the amount of LA [16,17]. The results of this study showed that IFPs changes between the fasciae might influence the outcome of the aQLB. Differences in IFPs and block levels between the right and left sides of the same patient suggest that other factors besides the relationship of the abdominal wall structures and BMI values with TLF may affect the IFPs. The results of this study may guide future studies on the mechanism of action of QLB and distribution of LA between the fasciae.