




INTRODUCTION
Aortocaval compression by the gravid uterus is a known physiological phenomenon that causes supine hypotension in full-term pregnant women [1]. Hypotension during spinal anesthesia may cause nausea and vomiting, and long-term severe hypotension may cause unconsciousness, pulmonary aspiration, hypoxia, acidosis, as well as fetal neurological injury due to reduction of uteroplacental blood flow [2]. Management of hypotension during regional anesthesia includes position change, fluid therapy, administration of vasopressors, and use of nonpharmacological methods [3]. Although position change using a tilt or a wedge is considered necessary, this management does not completely prevent hypotension resulting from aortocaval compression [4]. Neuraxial anesthesia blunts the cardiovascular compensatory mechanisms during cesarean delivery, and this may exacerbate maternal hypotension in the supine position. Additional factors, such as the size of the uterus, and maternal and fetal position, can be associated with aortocaval compression during neuraxial anesthesia [5]. Extensive paralysis of sympathetics and failure to relieve compression of the inferior vena cava could lead to a fatal fall in cardiac output [6].
This study aimed to investigate the differences, if any, according to the fetal position in the rate of hypotension by aortocaval compression with gravid uterus after spinal anesthesia during cesarean delivery.
MATERIALS AND METHODS
This single institutional prospective double-blind study was reviewed and approved by our hospital institutional review board, and informed consent was obtained from each patient.
In total, 71 American Society of Anesthesiology physical status classification I healthy patients with intrauterine pregnancy over 36 weeks of gestation who were scheduled for elective cesarean delivery under spinal anesthesia were enrolled in the study between August 24, 2017 and January 25, 2018. The exclusion criteria were cardiovascular or cerebrovascular disease, placenta previa, pregnancy-related hypertensive disease (systolic blood pressure greater than or equal to 150 mmHg), height < 150 cm or > 180 cm, weight < 50 kg or > 100 kg, known fetal abnormalities, fever, twin pregnancies, and diabetes mellitus.
In the operating room, fetal heart rate was monitored and fetal position was recorded by an obstetrician before spinal anesthesia was induced. When fetal heartbeat is detected using Doppler ultrasound fetal monitor, an ultrasound probe is fixated on the patientŌĆÖs abdomen where the best fetal heart signal can be obtained. If the probe is positioned to the right or left side of the midline of abdomen of the patient, the fetal position is considered on the right or left, respectively. Based on the fetal position, the patients were divided into two groups: fetal right position group (group R) and fetal left position group (group L).
Patients were not premedicated, and they were administered lactated RingerŌĆÖs solution at the full rate upon entering the operating room.
Patients in both groups were monitored using automated blood pressure-measuring devices, electrocardiography, and pulse oximetry on entering the operating room. After resting in the supine position for several minutes, the patients underwent noninvasive blood pressure measurements three times. The baseline systolic blood pressure (SBP) was calculated as the mean of three SBP recordings.
Spinal anesthesia was administered while the patient was in the left lateral position at the L3-4 or L4-5 vertebral interspace; 0.5% hyperbaric bupivacaine (10 mg) and fentanyl (15 ╬╝g) were injected intrathecally using a 25-gauge pencil-point needle (Pencan┬«, B/Braun, Germany). After the induction of spinal anesthesia, phenylephrine was infused at a rate of 50 ╬╝g/min in each group. Hypotension, defined as SBP Ōēż 80% of the baseline SBP despite phenylephrine infusion, was treated with a 100-╬╝g bolus of phenylephrine.
We measured the BP and heart rates (HRs) of the patients at 1-min intervals for 5 min and 2-min intervals after 5 min after the induction of spinal anesthesia until delivery, and at 5-min intervals for 30 min after delivery. Bradycardia was defined as HR < 50 beats/min and was treated with atropine (0.5 mg). After delivery, fetal body weight and Apgar scores at 1 and 5 min were recorded. Amniotic fluid index was also recorded. As a primary outcome measure, the number of patients who showed hypotension at least once was compared before delivery after spinal anesthesia. As a secondary outcome measure, the total infused doses of phenylephrine including bolus doses before delivery were compared.
Statistical analysis
In a pilot study, we compared the rate of hypotension between two groups before delivery by using the same methods as those used in this study. In total, 36 patients were enrolled, and the rate of hypotension was 70% (14 patients) in group R (20 patients) and 31% (5 patients) in group L (16 patients). The sample size for detecting significant difference in the rate of hypotension between two groups before delivery required to obtain a statistical power of 80% with an ╬▒ error of 0.05 was determined to be 30 patients in each group. Assuming a dropout rate of 10%, we enrolled 71 patients in this study.
Data are expressed as means ┬▒ SDs, medians (1Q, 3Q), or numbers (percentages).
Continuous variables such as SBP and HR were tested for normality using the Shapiro-Wilk test, and SBP was analyzed using two-way repeated measures ANOVA in one factor (following sphericity test) and HR, using Friedman repeated measures ANOVA on Ranks with DunnettŌĆÖs method for pairwise comparisons within each group. The StudentŌĆÖs t-test or Mann-Whitney rank sum test according to normality test were used for comparison of measurements (patient characteristics, outcome data) between the two groups. The rate of hypotension between the two groups was compared using the Žć2 test or FisherŌĆÖs exact test. Statistical analyses, and sample size and power calculations were performed using Sigma Stat version 4.0 (Systat Software Inc., USA). P values < 0.05 were considered statistically significant.
RESULTS
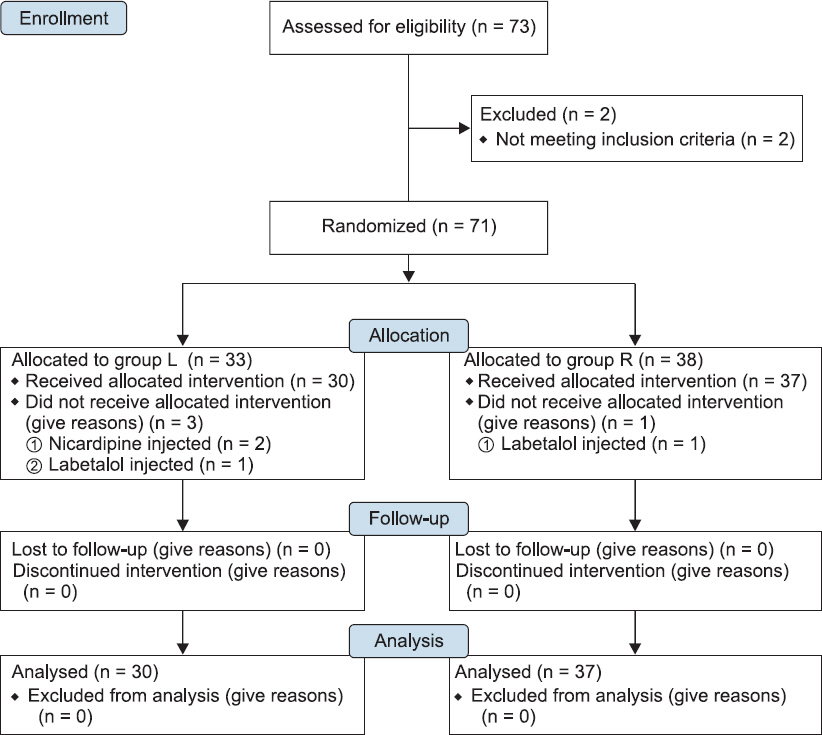
Four patients were excluded because they had elevated SBP above 150 mmHg. They were administered nicardipine or labetalol in the operating room before the induction of spinal anesthesia. A total of 67 patients were finally included in the study (Fig. 1). There were no statistical differences in the demographic data between the two groups (Table 1).
Table┬Ā1
Patient Characteristics
As primary outcome data, the rate of hypotension in group L was 40% (12 patients). Of the 12 patients, 6 patients showed hypotension only once, 4 patients showed hypotension twice, and 2 patients showed hypotension three or more times before delivery. The rate of hypotension in group R was 65% (24 patients). Of the 24 patients, 6 patients showed hypotension only once, 10 patients showed hypotension twice, and 8 patients showed hypotension three or more times before delivery. There was no significant difference in the rate of hypotension before delivery between the two groups (P = 0.075) (Table 2).
Table┬Ā2
Outcome Data
| Characteristics | Group L (n = 30) | Group R (n = 37) | P value |
|---|---|---|---|
| Sensory block height (coldness) | T4 (T3, T4) | T3 (T3, T4) | 0.301 |
| Hypotension before delivery | 12 (40) | 24 (65) | 0.075 |
| ŌĆāOnce | 6 (20) | 6 (16) | 0.935 |
| ŌĆāTwice | 4 (13) | 10 (27) | 0.285 |
| ŌĆāThree or more times | 2 (7) | 8 (22) | 0.166 |
| Phenylephrine dose before delivery (╬╝.g) | 308 (217, 375) | 375 (300, 467) | 0.028* |
| No. of patients with bradycardia | 3 (10) | 2 (5) | 0.650 |
| Time to delivery after SA (min) | 14.5 (13.0, 18.0) | 14.0 (13.0, 16.0) | 0.768 |
| 1-min Apgar score | 8 (8, 8) | 8 (8, 8) | 0.032* |
| 5-min Apgar score | 9 (9, 9) | 9 (9, 9) | 0.317 |
| Amount of infused fluid (ml) | 1,550 (1,325, 1,688) | 1,600 (1,500, 1,800) | 0.204 |
| Estimated blood loss (ml) | 700 (600, 900) | 700 (600, 800) | 0.758 |
The total phenylephrine dose required before delivery was significantly higher in group R (P = 0.028), and the 1-min Apgar score was significantly lower in group R (P = 0.032) (Table 2).
There were statistically significant decreases in SBP compared with the baseline values in both groups from 2 min after the spinal anesthesia; however, there was no significant difference in SBP between the groups (Fig. 2).
Fig.┬Ā2
Systolic blood pressure changes for 15 min after induction of spinal anesthesia. SBP: systolic blood pressure, Group L: left fetal position group, Group R: right fetal position group. *P < 0.05 compared with the baseline value in group L. ŌĆĀP < 0.05 compared with the baseline value in group R.

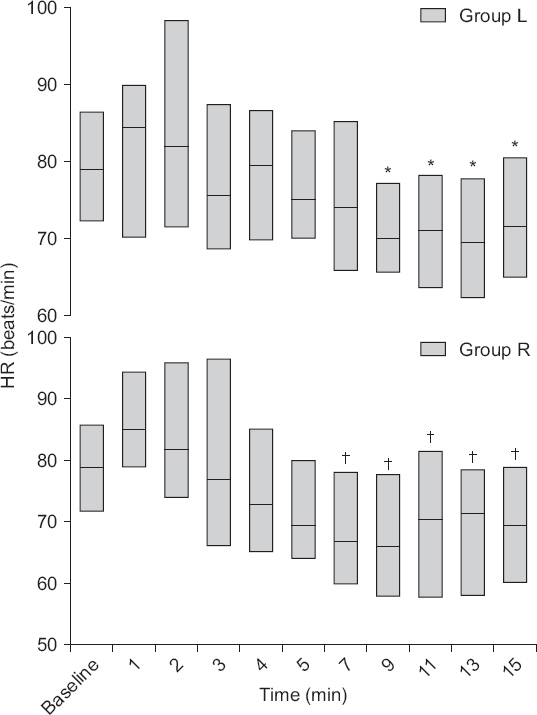
There were statistically significant decreases in HR compared with the baseline values in both groups from 7 or 9 min after the spinal anesthesia; however, there was no significant difference in HR between the groups (Fig. 3).
Fig.┬Ā3
Heart rate changes for 15 min after induction of spinal anesthesia. HR: heart rate, Group L: left fetal position group, Group R: right fetal position group. The boxes represent the median (black middle line) limited by the 25th (1Q) and 75th (3Q) percentiles. *P < 0.05 compared with the baseline value in group L. ŌĆĀP < 0.05 compared with the baseline value in group R.
DISCUSSION
This study showed that supine hypotension occurred in 36 of the 67 enrolled patients. More than half of the healthy patients (54%) who underwent cesarean delivery under spinal anesthesia despite efforts to maintain the baseline hemodynamics showed hypotension before delivery. The rate of hypotension in group R (65%) and group L (40%) was not statistically different (P = 0.075).
Although there is a marked reduction of systemic vascular resistance at the moment of delivery, an increase in the cardiac output is enough to compensate the reduction; consequently, the mean arterial pressure remains stable in healthy patients [7]. In our study, arterial vasodilation induced by spinal anesthesia occurred in women with aortocaval compression by gravid uterus. However, shortage of cardiac output compensation may have caused a significant decrease in the SBP compared to baseline in group R from 2 min after the spinal anesthesia until delivery. In group L as well, SBP was significantly decreased compared to baseline from 2 min after the induction of spinal anesthesia; however, cardiac output compensation may have likely occurred at 13 min after the spinal anesthesia. However, there was no significant difference in the SBP between the groups. The amount of fluid infusion and blood loss also did not show significant difference between the groups.
The heart rate of patients in both groups was significantlydecreased compared with the baseline values. We attribute this to reflex bradycardia due to phenylephrine [8]. However, there was no significant difference between HR in the two groups. These results show that hemodynamic changes according to the fetal position do not differ until delivery.
The one-min Apgar score was significantly lower in group R than in group L (P = 0.032). Greater hemodynamic instability can affect uteroplacental blood flow [2], considering aortocaval compression by gravid uterus and additive spinal sympathetic blockade. However, it did not clinically differ between the two groups, as they showed the same Apgar score.
Administration of medications that increase the uterine tone is important to prevent postpartum hemorrhage; however, the usual first-line treatment, oxytocin, may put the woman in labor at risk of hypotension owing to its prominent vasodilatory effect [9,10]. Even under spinal anesthesia for cesarean delivery, patients may secrete endogenous oxytocin in response to the presence of the newborn baby [11]. Langesaeter et al. [12] reported that delivery may contribute to the circulatory changes, but the main effects are due to oxytocin. As the main focus of this study is on the hemodynamic effects of the fetus before delivery, studies on the hemodynamic effects of oxytocin will be conducted later.
In this study, patients were placed in the supine position after the induction of spinal anesthesia without 15┬░ left tilt using right lumbar-pelvic wedge. According to a recent report, maternal supine position during planned cesarean delivery under spinal anesthesia in healthy term women does not impair neonatal acid-base status compared to the 15┬░ left tilt position, when both a crystalloid co-load and a phenylephrine infusion are used to maintain the baseline maternal SBP [13]. Moreover, Sohn et al. reported that there was no difference in hypotension between lateral position and supine position during cesarean delivery following spinal anesthesia [14]. We designed this study for balancing the effect of fetal position, and the patients needed to be positioned without tilting. Healthy patients were enrolled and crystalloid co-load with phenylephrine infusion was followed to prevent supine hypotension. This study was limited by potential errors in the measurement of fetal position with Doppler ultrasound fetal monitor; further research to reduce such errors is warranted.
In conclusion, there was no difference according to fetal position in the number of patients who showed hypotension before delivery after spinal anesthesia. However, a significantly higher total phenylephrine dose for maintaining hemodynamic stability before delivery was required in group R. However, further research on the optimal phenylephrine dose is necessary to confirm this finding.




