




INTRODUCTION
Endotracheal intubation and extubation accompanied by general anesthesia induce various effect on patient. It may cause hemodynamic response which result in increase of arterial blood pressure and heart rate. This response was associated with sympathetic stimulation caused by airway irritation. And it can cause a stress situation that may cause an adverse event in some susceptible patients [1].
Respiratory complications after tracheal extubation are more common than during intubation and induction of anesthesia [2]. Coughing due to airway irritation during extubation can cause harmful effects such as hypertension, tachycardia, arrhythmia, bronchospasm, bleeding at operative site. In addition bucking and coughing frequently occurred during extubation may lead to an abrupt increase in intraocular pressure, intrathracic pressure, intraabdominal pressure, and intracranial pressure. These can increase the mortality and morbidity of the patient [1,3]. Therefore, efforts should be made to prevent the adverse events and poor outcomes that may occur in patients who are vulnerable to stress by appropriately controlling stimuli.
Lidocaine administered to the larynx or trachea is known to be effective in suppressing blood pressure increase caused by intubation [4,5], and is also known for blocking cardiovascular responses to airway irritation. Based on the previous studies, the aim of this study was to investigate the effect of 1% lidocaine administered intratracheally on airway response and hemodynamic response during emergence and time of extubation.
MATERIALS AND METHODS
After obtaining approval from the Institutional Review Board of our institution (IRB no. DKUH 2017-07-004-001) and informed consent from patients, we investigated a total of 60 patients at a single academic medical center. The patients with physical status American Society of Anesthesiologists classes from I to III who were aged 18-60 years, scheduled to undergo elective surgery under general anesthesia, were included in this study. Patients with a history of allergy to local anesthetics, cardiovascular or respiratory disease, recent upper respiratory infection, laryngeal or tracheal pathology and being judged inappropriate for participation by researcher were excluded.
The patients were randomly divided into two groups of thirty patients with L group receiving intratracheal 1% lidocaine, N group receiving intratracheal placebo. L group was given 1% lidocaine 0.5 mg/kg by endotracheal administration. The other group, group N, the placebo group received the same volume of normal saline by the same route. The number of cough, sore throat numerical rating score (NRS), incidence of local anesthetic systemic toxic reaction, laryngospasm, and hoarseness was recorded. In addition, the number of coughs were count according to three levels by its severity, and it was converted into an indicator of cough score.
Anesthesia was induced with propofol 2 mg/kg and fentanyl 2 ┬Ąg/kg. Rocuronium 0.6 mg/kg was administered to facilitate endotracheal intubation. Intubation was performed 3 min after rocuronium injection with laryngoscope by researcher A. The size of the endotracheal tube was 7.5 mm inside diameter for male and 7.0 mm inside diameter for female. After air ballooning of endotracheal tube and confirming the depth by auscultation, tube was fixed 1-2 cm above the carina. Anesthesia was maintained with a mixture of oxygen and medical air with Desflurane, which was controlled within the range of 6-9 vol% until the end of surgery. At the end of surgery, the researcher A recorded the hemodynamic index and then administered the prepared study drug to the endotracheal tube according to the patient group to which the patient determined in the randomization. When injecting the drug into the tube, 1% lidocaine, a dilute solution made by mixing 2% lidocaine with saline at a ratio of 1: 1, was administered with a dose of 0.5 mg/kg along the inner side of the tube at a rate of 1 ml/s. After administration of the drug, the other anesthesiologist entered the operating room and then discontinued Desflurane and ventilated with 100% O2 at a rate of 8 L/min. When the concentration of the inhalation anesthesia is lowered to less than 0.1 minimum alveolar concentration and the patient starts to move, neostigmine 0.04 mg/kg, glycopyrrolate 0.008 mg/kg or neostigmine 0.04 mg/kg and atropine 0.02 mg/kg were administered intravenously to reverse muscle relaxation. To minimize airway irritation, no aspiration through the endotracheal tube was performed and the patient did not wake or stimulate the patient until the patient started moving on their own. Extubation was performed after the patientŌĆÖs consciousness was restored to the degree required and the spontaneous breathing remained stable. Thereafter, hemodynamic index was recorded, and complications including general anesthesia were observed. Thereafter, hemodynamic parameters were recorded, and complications including general anesthesia were observed. After extubation, the researcher B observed the number of coughs which was divided into three stages according to the severity of the cough. The severity of cough was assessed as the three-category scale for scoring cough used Ki et al. [6]. At this time, only the researcher B performed the evaluation of the cough for the consistency of the severity and frequency of cough. The score of cough was calculated with weighting according to the severity. The formula for calculating the cough score in this study is as follows:
The score of sore throat was assessed by NRS. After arriving the postanesthetic care unit (PACU), the patient was asked to respond separately to the pain of surgical site. In addition, the presence of hoarseness, the presence of local anesthetic toxicity, and the presence or absence of laryngospasm were observed until the patients leaved PACU to ward.
In the present study, the sample size was calculated ausing the following method. Based on the results of the pilot study and the anticipation of a 20% difference between the two groups, 27 patients were required in each group with a type 1 error of 0.05 and a power of 0.8. Considering a possible dropout rate of 10%, per group 30 patients were needed. Therefore, the total sample size was 60. All values are expressed as mean ┬▒ standard deviation, median and interquartile range, or number and percentage. Dermographic data, value and changes of hemodynamic parameters were analyzed by the independent t-test and the chi-square test. Mann-Whitney U test was used for the analysis of the frequency of cough, the cough score, and the sore throat score, because the data did not satisfy the normal distribution. In addition, logistic regression analysis was also performed by analyzing cough and sore throat according to the occurrence of cough and sore throat. The differences in blood pressure and heart rate before and after extubation were compared by linear regression analysis. All statistical analyses were performed using PASW statistics 18.0 for windows (IBM, USA), and they were considered statistically significant when the P value was less than 0.05.
RESULTS
The characteristics of 60 patients are shown in Table 1. There was no difference of demographic data between the two groups, L group and N group. However, in the L group, the mean diastolic blood pressure before induction of anesthesia was lower than that of N group (Table 1).
Table┬Ā1
Clinical Characteristics of Patients
| Variable | Total (n = 60) | N group (n = 30) | L group (n = 30) | P value |
|---|---|---|---|---|
| Sex, male | 34 (56.7) | 19 (63.3) | 15 (50.0) | 0.435 |
| Age (yr) | 42.5 ┬▒ 10.9 | 43.9 ┬▒ 10.1 | 41.1 ┬▒ 11.7 | 0.324 |
| ASA classification | ||||
| ŌĆāI | 39 (65.0) | 16 (53.3) | 23 (76.7) | 0.092 |
| ŌĆāII | 19 (31.7) | 12 (40.0) | 7 (23.3) | |
| ŌĆāIII | 2 (3.3) | 2 (6.7) | 0 (0.0) | |
| Smoking history | ||||
| Current smoker | 45 (75.0) | 22 (73.3) | 23 (76.7) | 1.000 |
| Anesthesia time (min) | 120.0 (88.8, 161.3) | 127.5 (86.3, 163.8) | 102.5 (90.0, 153.8) | 0.824 |
| Hemodynamic index before the induction of general anesthesia | ||||
| ŌĆāSBP (mmHg) | 118.6 ┬▒ 24.4 | 112.9 ┬▒ 20.9 | 124.2 ┬▒ 26.7 | 0.075 |
| ŌĆāDBP (mmHg) | 68.6 ┬▒ 15.3 | 64.5 ┬▒ 12.7 | 72.7 ┬▒ 16.7 | 0.036* |
| ŌĆāHR (beats/min) | 76.2 ┬▒ 15.9 | 74.6 ┬▒ 16.2 | 77.8 ┬▒ 15.7 | 0.440 |
| Local anesthetics toxicity | 0 (0) | 0 (0) | 0 (0) | |
| Laryngospasm | 0 (0) | 0 (0) | 0 (0) | |
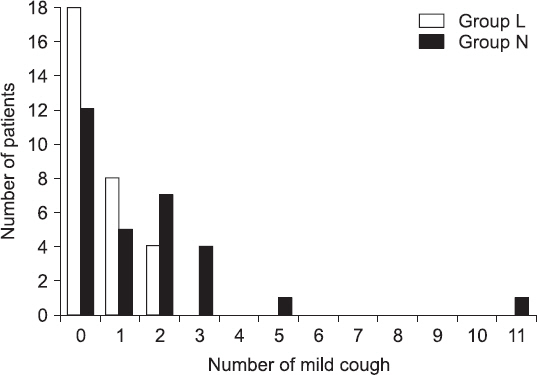
The frequency of cough, value of cough score and the severity of sore throat was less in the L group than in the N group. According to severity of cough, the frequency of mild cough was dominant in the L group (Fig. 1). And the value of cough score and sore throat score were significantly different in the L group compared to the N group (Table 2).
Table┬Ā2
Number of Coughs according to the Severity and Score of Cough and Sore Throat
| Variable | Total | N group | L group | P value |
|---|---|---|---|---|
| Mild cough | 0.50 (0.00, 2.00) | 1.00 (0.00, 2.00) | 0.00 (0.00, 1.00) | 0.022* |
| Moderate cough | 0.00 (0.00, 0.00) | 0.00 (0.00, 0.00) | 0.00 (0.00, 0.00) | 0.115 |
| Severe cough | 0.00 (0.00, 0.00) | 0.00 (0.00, 0.00) | 0.00 (0.00, 0.00) | 0.154 |
| Cough score | 1.00 (0.00, 2.00) | 1.00 (0.00, 3.00) | 0.00 (0.00, 1.00) | 0.017* |
| Sore throat | 0.00 (0.00, 4.00) | 3.00 (0.00, 5.75) | 0.00 (0.00, 2.00) | 0.011* |
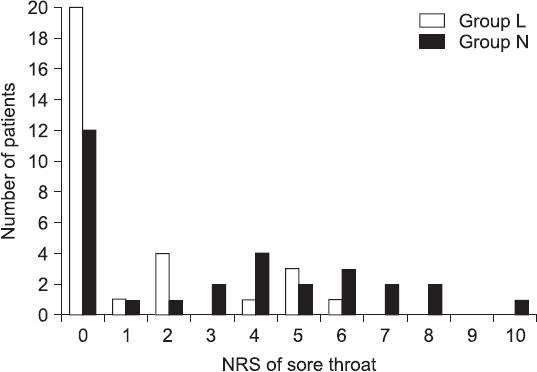
The number of patient according the sore throat score was shown in Fig. 2. The number of patients who had a low score of sore throat was more in N group than L group.
Fig.┬Ā2
Number of patients according to sore throat severity in each group. NRS: numerical rating score.
The odds ratios for the occurrence of cough and sore throat were 0.28 and 0.21, respectively, in L group compared to N group. The patient who showed hoarseness was not found in the L group (Table 3).
Table┬Ā3
Differences in Complication Occurrence between the Two Groups
| Variable | L group (reference: N group) | ||
|---|---|---|---|
| Odds ratio | 95% confidence interval | ||
| Lower limit | Upper limit | ||
| Hoarseness | 0.00 | ||
| Cough | 0.28 | 0.08 | 0.90 |
| Sore throat | 0.21 | 0.06 | 0.70 |
The hemodynamic parameters of systolic blood pressure, diastolic blood pressure, and heart rate after emergence increased compared to those of before emergence. In the L group, there were statistically significant decrease in difference of diastolic blood pressure than in the N group, and there were also difference of systolic blood pressure change than the N group (Table 4).
Table┬Ā4
Differences in Hemodynamic Changes between the Two Groups
| Variable | L group (reference: N group) | ||
|---|---|---|---|
| Β | Standard error | P value | |
| ΔSBP | -14.8 | 7.7 | 0.061 |
| ΔDBP | -10.4 | 5.2 | 0.050* |
| ΔHR | -6.4 | 4.9 | 0.195 |
Group variable was explanatory (independent) variable. Each model was adjusted for sex, age, American Society of Anesthesiologists classification and smoking history. B: gradient, SBP: systolic blood pressure, DBP: diastolic blood pressure, HR: heart rate. ΔSBP = SBP after extu- bation - SBP before emergence, ΔDBP = DBP after extubation - DBP before emergence, ΔHR = HR after extubation - HR before emergence of anesthesia.
In both groups, there were no adverse event such as systemic toxic reaction of the local anesthetics or pulmonary aspiration or laryngospasm.
DISCUSSION
In the present study, intratracheally administration of 1% lidocaine reduced occurrence of mild cough, the score of cough and sore throat caused by airway irritation during extubation. Moreover, the elevation of arterial blood pressure and heart rate was suppressed.
Endotracheal intubation associated with general anesthesia causes complications, such as cough and sore throat after emergence. Approximately 14.4-50% of the patients presented with cough and sore throat after intubation [7], and various efforts have been made to reduce these complications. Bagchi et al. [8] injected dexamethasone intravenously after intubation, and Zhao et al. [9] administered remifentanil to reduce sore throat and cough. In addition, Soares et al. [10] attempted to inflate the balloon of the endotracheal tube with lidocaine, and Jee and Park [5] and Bilotta et al. [11] reported the usefulness of lidocaine intratracheal instillation. However, there is no consensus on which of these methods is the most superior.
In the present study, we use 1% lidocaine administered intratracheally. There are not many studies about the proper concentration of lidocaine intratracheally administered. When a high concentration of lidocaine is used for intratracheally administration, there may be a risk of systemic toxicity due to overdose of local anesthetics. Considering that acidic substances generally cause more severe aspiration pneumonia [12], the possibility of aspiration pneumonia caused by an acidic solution, such as lidocaine (a weak acid) that is administered at a high concentration in the trachea cannot be ruled out. Frank and Lalonde [13] reported that 1% lidocaine was slightly more neutral than 2% lidocaine, thus 1% lidocaine, which is mildly acidic and more diluted than 2% lidocaine, might be less irritating to the mucosa of the trachea. Moreover, less systemic toxic reactions are also expected. Therefore, in this study, we tried to reduce the adverse effects of intubation with 1% lidocaine, which had a lower concentration than 2% lidocaine, which was used in previous studies. Systemic toxicity due to local anesthetics and aspiration pneumonia did not occur in our study.
We considered that the mechanism associated with the attenuation of airway stimuli and hemodynamic responses by intratracheally administration of lidocaine may be interpreted as an increase in blood concentration due to systemic absorption of the drug or the anesthetizing effect of the topical mucosa. Lidocaine may be rapidly absorbed into the circulation from the tracheobronchial tree with the same or lower blood concentrations after an intravenous injection [14]. In addition, lidocaine administered via the trachea may spread distally due to gravity when a patient is in supine position, and it may be attributed to the anesthetizing effect of mucosa. We found that the incidence of cough was lower in the L group who received 0.5 mg/kg of 1% lidocaine intratracheally than the N group. Particularly, the frequency of cough was assessed separately according to the severity of cough. In the L group, the incidence and frequency of mild cough was lower.
In the present study, the incidence and score of sore throat were also lower in L group administered 1% lidocaine 0.5 mg/kg intratracheally than N group. Although intratracheal administration of lidocaine can be a useful method in attenuating airway irritation due to an endotracheal tube, results of sore throat in previous studies have been conflicting. Herlevsen et al. [15] showed that there was no significant correlation between lidocaine and incidence of postoperative sore throat. Moreover, Klemola et al. [16] reported that lidocaine increased the incidence of postoperative sore throat. Conversely, Oh et al. [17] reported that preoperative pharyngolaryngeal and intratracheal spraying with 10% lidocaine reduces the incidence of postoperative sore throat. In the present study, we considered that our result was due to the effect of systemic absorption of lidocaine. However, further studies on the mechanisms are required.
Although not statistically significant, changes in blood pressure and heart rate were more stable. However, regarding diastolic blood pressure, a difference was observed between the two groups before the induction of anesthesia, and further studies are required to validate the stability of the hemodynamic parameters.
The present study had some limitations. First, the total number of patients was 60, which is insufficient for a stratified analysis adjusted for various parameters. Second, it is not possible to accurately administer the drug to the area around the balloon of the endotracheal tube, which can cause the most severe irritation in endotracheal tube insertion. Third, regarding diastolic blood pressure, a difference was already observed in the measured value before the induction of anesthesia, and it was difficult to compare such value with the postoperative value. Therefore, this value was replaced by comparing the blood pressure before the induction of anesthesia with the value after induction. Fourth, the volume of lidocaine administered intratracheally in our study was not enough to cause aspiration pneumonia, the study regarding the volume of lidocaine that cause aspiration pneumonia might be needed. Lastly, when administrating lidocaine into the trachea, an accurate method of administration may have an effect on the result. Efforts in evaluating these methods might be needed to improve the accuracy of administration to maximize the local anesthetic effect near the balloon, which is the area where the most stimulation is expected.
Despite these limitations, our study showed that endotracheal administration of 1% lidocaine can be safely and effectively used to reduce the airway response and hemodynamic response during emergence and time of extubation through randomization and double-blind method, and these results are consistent with those of previous studies [5,11]. In addition, most of the existing studies did not categorize the severity of cough but simply measure the number of coughs, however, in the present study, cough was divided into three categories according to their severity. Moreover, it is meaningful that the severity of cough was evaluated with a new indicator of cough score.
In conclusion, the endotracheal administration of 1% lidocaine is effective in reducing cough and sore throat caused by extubation.




